 Home
Home
"On Chloroform and Other Anæsthetics"
Edited by Benjamin Ward Richardson
(October 1858)
[Finished third pass on proofreading text. It is a massive task to digitize so large a volume into running, searchable text. If you find something that seems amiss, chances are that it is; please send me a message (vintenjo@msu.edu) and I will check text on the web site against the originals, correct if necessary, and send you a note of appreciation.
Pagination breaks are noted in square brackets. Pharmacy symbols are given in closest approximation in UTF-8 Unicode, when available; all are explained in square brackets. I have deleted the period after per cent. Otherwise, searchable text replicates the original volume.
Users of Mozilla Firefox on Windows XP and Windows Vista should no longer experience a text blackout partially through this file; a graphic designer at MATRIX has adjusted the background to overcome this problem. There have never been problems when the file is displayed in Internet Explorer or Firefox run on Windows 7 --PVJ.]
The book here presented to the reader is the legacy to science of Dr. John Snow. The completion of the work was his last act and deed. In editing the book, therefore, all that remained to be done consisted in the construction of the index, and in this a plan suggested by the author himself has been followed.
In contributing the memoir, I have performed a painful and unexpected duty: the fulfillment of a promise given at a moment when two friends who often enjoyed close companionship met at one of their happiest meetings. The promise was given with the idea of fulfillment far distant, or improbable altogether, and, as connected with a more extended biographical survey, reserved for the work of years long in the future; it is called for now hastily and in deep sorrow. [iii/iv]
Writing with the fact of my late friend's death not as yet fully realized; with the sensation still on me at intervals (like one who has lost a part of his own body, and yet at times conceives the lost present), that he cannot possibly be so far away; I may perchance be pardoned for any deficiencies in style or matter. I have done my best, and leave it so.
B. W. Richardson.
12, Hinde Street, Manchester Square [London].
August 6th, 1858.
[The book was not published until October, as the following advert in the October 1858 issue of Sanitary Review and Journal of Public Health suggests:
Snow was felled by a stroke on 10 June 1858. He died on the 16th. His Last Will and Testament, from August 1857, made brothers William and Robert executors. William Snow "proved" the will on 8 July 1858, Robert Snow some time afterward. One, or both of them, must have given Richardson access to Snow's papers so that he could shepherd On Chloroform through publication and write a biographical memoir. What happened to those papers thereafter is unclear. They have yet to resurface.]
[following table of contents appears on pp. v-viii]
Click here for a PDF copy of Benjamin Ward Richardson's "Memoir of the Author," The Life of John Snow, M.D.
Click here for a PDF copy of Benjamin Ward Richardson's Index which he prepared after Snow's death.
[Notes in the original appear as footnotes. We decided to transform the footnotes into endnotes, rather than imbed the notes in the text (the norm in other documents in the Snow's Works portion of the web site) for anyone who wishes to review them in their entirety--PV-J.]
The most important discovery that has been made in the practice of medicine since the introduction of vaccination, is, undoubtedly, the power of making persons perfectly insensible to the most painful surgical operations, by the inhalation of the vapours of ether, chloroform, and other agents of the same kind.
In giving a brief outline of this discovery, it is necessary to inquire into the attempts of every kind which had previously been made to prevent severe pain; and also to notice the history of medicinal inhalations, whether undertaken with the view of preventing pain, or of relieving or curing disease.
The practice of taking opium and other vegetable narcotics, to relieve pain or procure sleep, was common in the most remote periods to which history extends but the earliest notices which remain of any attempts to prevent the pain of surgical operations were written at the period of the Roman Empire. They were alluded to by Dr. Simpson at the Medico-Chirurgical Society of Edinburgh in November, 1847.1
Dioscorides,2 speaking of mandragora, says, "Some persons boil the root in wine down to a third part, and preserve the decoction, of which they administer a cyathus (rather more than an ounce and a half) in want of sleep and severe pains of any part, and also before operations with the [1/2] knife or the actual cautery, that they may not be felt." (Ante sectiones ustionesve, ut ne sentiantur.) Further on he says: "A wine is prepared from the bark of the root without boiling, and three pounds of it are put into a cadus (about eighteen gallons) of sweet wine, and three cyathi of this are given to those who require to be cut or cauterized: when being thrown into a deep sleep they do not feel any pain."
The same author also adds,3 in speaking of a kind of mandragora called morion, "They relate that a drachm of it being taken as a draught, or eaten in a cake or other food, causes infatuation, and takes away the use of the reason. The person sleeps without sense, in the attitude in which he ate it, for three or four hours afterwards. Medical men also use it when they have to resort to cutting or burning."
In treating of mandragora, Pliny3a remarks that the juice of the leaves is more powerful than the preparations made from the root. He says, "Some persons even die from a considerable draught. It has the power of causing sleep in those who take it. The dose is half a cyathus (six drachms). It is taken against serpents, and before cuttings and puncturings, lest they be felt. For these purposes it is sufficient for some persons to have sought sleep from the smell (of the medicine)."
Apuleius3b under the head mandragora, says, "If any one eat it he will immediately die, unless he be treated with butter and honey, and vomit quickly. Further, if any one is to have a limb mutilated, burnt, or sawn, he may drink half an ounce with wine, and whilst he sleeps the member may be cut off without any pain or sense."
After reading the above passages from such well-known authors, it may be asked how it was that the practice of [2/3] preventing the pain of surgical operations was entirely unknown just prior to 1846. The reason, no doubt, was that the statement these passages contain was looked upon as a vulgar error of the period, which had imposed on the credulity of the authors. Dr. Woodville,4 speaking of the use of mandragora by the ancients, says, "They employed it principally in continue watchings, and in those more painful and obstinate affections which were found to resist less powerful medicines." He gives, in a foot note, a reference to the place in Dioscorides from which the passages above quoted are taken, and had he believed in the performance of operations without pain, we may conclude he would not have passed over so important a fact in silence.
With the knowledge we at present possess, however, a different view must be taken of the subject; and it must at least be allowed that the statements of the ancients had some foundation in truth. This is rendered more certain by the circumstance that atropa mandragora belongs to the same genus as belladonna, which has a greater power in annulling the common sensibility than any plant in present use, unless it be aconite. The loss of reason, described by Dioscorides as caused by mandragora, is a striking symptom of poisoning by the class of plants (the solanaceæ) to which it belongs. It appears from some remarks of Aretæus5 and Cælius Aurelianus5a that people were in the habit of taking mandragora as an inebriating agent in the time of the ancients, as an allied plant, the datura, is used at present by the natives of India. This practice would lead to a correct knowledge of the quantity which might be taken with impunity.
The mandrake is scarcely used in medicine at present, but [3/4] its narcotic properties are well established. Hoffberg6 administered the root in doses of three grains in some cases of gout, with the effect of relieving the pain.
Cases of poisoning by belladonna end, with very few exceptions, in recovery, however large the dose, and however alarming the symptoms may be; and, taking all the above circumstances into account, it is probable, that after ascertaining the right quantity to be administered for the purpose, this medicine or mandragora might be used, with considerable success, and no great danger, to prevent the pain of operations, if chemistry had not supplied us with agents much more convenient.
Not many ages after the Greek and Roman authors above quoted were describing the effects of mandrake in preventing the pain of operations, another plant, the Indian hemp, was employed for the same purpose in a more remote part of the world. M. Stanislas Julien, in an article on Chinese Medicine7 gives a notice of a work entitled Koukin-i-tong, or a General Collection of Ancient and Modern Medicine, in fifty volumes, 4to., and makes an extract from it respecting Hoa-tho, a practitioner, who flourished under the dynasty of Wei, between 220 and 230 of our era. Respecting Hoa-tho, it is stated that--"When he found that it was necessary to employ acupuncture, he applied it in two or three places; he did the same with the moxa, if it was indicated by the nature of the affection which he had to treat. But if the malady was situated in parts on which the needle, the moxa, or liquid medicines could not act--for example, in the bones, in the medulla of the bones, in the stomach, or the intestines, he gave to the patient a preparation of hemp (Ma-yo), and, at the end of some instants, he became as insensible as if he had been drunk, or deprived of life. Then, [4/5] according to the case, he made openings and incisions, performed amputations, and removed the cause of mischief; he then brought together the tissues with points of suture, and applied liniments. After a certain number of days (at the end of a month, according to the annals of the later Hân) the patient found himself re-established, without having experienced the slightest pain during the operation."
We are not informed of the way in which the hemp was administered. If insensibility was caused so quickly, as is stated, it must have been by inhaling the fumes of the hemp when exposed to heat, and not by taking it into the stomach. This view of the matter is rendered more probable by the circumstance that the ancient Scythians were in the habit of inhaling the fumes of hemp,8 several centuries before the time of Hoa-tho, and also by the practice of the Hindoos at present, who inhale the fumes of hemp from a pipe. The remark that the patient became re-established at the end of a certain number of days, must refer to his recovery from the wound caused by the operation, and we are not informed how long the state of insensibility continued.
The next notice of any attempt to prevent the pain of operations, that I am aware of, occurs in the work on Surgery of Theodoric, an author who lived in Italy in the latter half of the thirteenth century. He writes as follows:9 "The making of a flavour for performing surgical operations according to Dominus Hugo. It is thus made:--take of opium, of the juice of the unripe mulberry, of hyoscyamus, of the juice of hemlock, of the juice of the leaves of mandragora, of the juice of the woody ivy, of the juice of the forest mulberry, of the seeds of lettuce, of the seeds of the dock, which has large round apples, and of the water hemlock (cicuta)--each an ounce; mix all these in a brazen vessel, [5/6] and then place in it a new sponge; let the whole boil, as long as the sun lasts on the dog days, until the sponge consumes it all, and it is boiled away in it (the sponge). As oft as there shall be need of it, place this sponge in hot water for an hour, and let it be applied to the nostrils of him who is to be operated on, until he has fallen asleep; and so let the surgery be performed. This being finished, in order to awaken him, apply another sponge, dipped in vinegar, frequently to the nose, or throw the juice of the root of fenugrek into the nostrils; shortly he awakes."
I altogether disbelieve that a sponge, prepared as above, would, after being placed in hot water, give off any odour or vapour which would cause insensibility. The active ingredients, as they exist in the various plants, are not sufficiently volatile to be given off at a heat below that of boiling water. Hemlock, indeed, contains a volatile principle, which can be liberated by an alkali; but, even if it were set free by any chance during the preparation of the sponge, it would all be dissipated by the long boiling.
If sleep were really caused in this way, it must have been by some of the moisture from the sponge reaching the mouth or throat, and being swallowed; and it may be remarked that the author speaks of the preparation of a taste or flavour, (confectio saporis), rather than an odour, although the sponge is certainly directed to be applied to the nostrils. It must be remarked, also, that if the patient were made so insensible, as not to feel the surgeon's knife, he would be little affected by vinegar, or the juice of fenugrek, in his nostrils.
Immediately after the prescription quoted above, and in the same paragraph with it, Theodoric gives another recipe from Master Hugo, directing antimony, quicksilver, soap, quick lime, and a little arsenic, to be sublimed together. A portion of the resulting compound, the size of a nut, is [6/7] directed to be placed over a hernia, or whatever else is to be operated on. Then follows a rather lengthy direction for subliming arsenic, also from Dominus Hugo. The arsenic so sublimed is described as rendering surgical operations extremely pleasant. The words are--"hæc acus fiat mitis et suavis: sicut sudor beatæ virgins quum peperit Christum."
I have applied arsenic to the skin for twenty-four hours, with no other effect than irritation, and an eruption of pimples, the sensibility of the part being increased; and in my opinion, arsenic would not cause insensibility, unless it were applied so long that the inflammation caused by it should end in gangrene. I consider that the statement of Theodoric, respecting arsenic, strengthens the doubts I have expressed concerning his spongia somnifera. There is another reason for disputing the efficiency of the above mentioned recipes. Theodoric directs the patients about to undergo operations to be tied, or held by strong men. In the operation for hernia, for instance, he directs the patient to be tied to the bench, or table, with three bands, one round the ankles, another round the thighs, and a third across the chest, holding the arms and hands. This circumstance is the more significant, since Theodoric had lived some time with Hugo, and seen his practice, as he states in the dedication to his work.
It is reasonable also to conclude that if any successful plan of preventing the pain of surgical operations had been introduced after the revival of literature, it would not have fallen into disuse and been forgotten.
In an interesting paper by Dr. Silvester,10 an anecdote is quoted, with an intention to show that anæsthetics were commonly had recourse to in severe operations as late as the end of the seventeenth century. The quotation is from [7/8] a German work by A. G. Meissner, called Skizzen, or Sketches, and published at Carlsruhe in 1782. It is as follows:--
"Augustus, King of Poland and Elector of Saxony, suffered from a wound in his foot, which threatened to mortify. The court medical men were opposed to the operation of amputation; but during sleep, induced by a certain potion surreptitiously administered, his favourite surgeon, Weiss, a pupil of Petit, of Paris, cut off the decaying parts. The royal patient was disturbed by the proceeding, and inquired what was being done, but on receiving a soothing answer he again fell asleep, and did not discover till the following morning, after his usual examination, that the operation of amputation had really been performed."
It is most probable that the potion surreptitiously administered in this case, was an ordinary sleeping draught, and that only the "decaying parts" were cut off, as in fact is stated. The decaying parts of course would be without feeling.
The mind of surgeons seems now and then to have turned spontaneously towards preventing or alleviating the pain of operations, and certain attempts and suggestions were made with this object during the later part of the last century, in apparent ignorance of what had been done by the ancients in this direction.
Ambroise Tranquille Sassard, principal surgeon of the Hospital la Charité at Paris, recommended the employment of a narcotic previous to serious and painful operations, the dose to be proportioned to the age and strength of the patient.11 He does not state whether the plan was actually tried.
Mr. James Moore, surgeon,12 recommended compression [8/9] of the large nerves, and tried it on a patient in St. George's Hospital, whose leg Mr. John Hunter amputated below the knee. The crural and sciatic nerves were compressed for nearly an hour by an instrument contrived for the purpose, and Mr. Moore considered that the greater part of the pain was prevented. The patient complained more of the sawing of the bone than of the cutting part of the operation. I am not aware whether this plan was tried in other instances, but it is certain that it did not come into general use.
M. le docteur Liégard (de Caen) has stated,13 that the peasants in his part of France are in the habit of tying a band very tightly round the arm or leg before operations on the extremities. He had himself removed a toe nail in two cases, without pain, after a handkerchief had been tied very tightly round the lower part of the leg. By this measure both the nerves and blood vessels are, of course, more or less compressed.
The persons who believe in the existence of a force or power, which they call Mesmerism, or animal magnetism, made many and persevering efforts in recent times to cause insensibility to the surgeon's knife. In some cases they were imposed on by dishonest and designing patients, who afterwards confessed they had suffered the pain to which they had pretended to be insensible, but in other cases I have no doubt of the operations having really been performed without pain. Absence of consciousness and sensation is a common symptom in many cases of hysteria and catalepsy, and in certain susceptible persons, hysteria and catalepsy, or conditions nearly resembling them, can be induced by acting on the imagination, or by exhausting the attention by means of the fixed stare and monotonous "passes" of the so called Mesmerisers. [9/10]
Dr. Esdaile was more successful in putting Hindoos to sleep, and operating on them in the hypnotized14 state, than any one has been with Europeans: yet it was only in a portion of the cases in which it was tried that the alleged agent took effect. In many instances, efforts continued for two or three months had no effect on the patient; and in many of the operations, which were reported as successful, "there was much convulsive movement of the limbs, corrugation of the brows, and even loud cries and sobs," although the patients afterwards denied all knowledge of what had passed.15
The discovery of the means of preventing pain, which will occupy the greater number of the following pages, did not arise out of any of the attempts either in ancient or modern times above enumerated. It sprung directly from the practice of inhaling chemical and medicinal substances.
The custom of inhaling the fumes of narcotic plants existed at the very commencement of the historic period, as appears by the following passages from Herodotus. Speaking of the people who inhabited some small islands on the river Araxes, which flows into the Caspian Sea, he says,16 "They add that they have discovered other trees that produce fruit of a peculiar kind, which the inhabitants, when they meet together in companies, and have lit a fire, throw on the fire as they sit round in a circle; and that by inhaling the fumes of the burning fruit that has been thrown on, they become intoxicated by the odour, just as the Greeks do by wine; and that the more fruit is thrown on, the more intoxicated they become, until they rise up to dance and betake themselves to singing." [10/11]
Again, when treating of the funeral ceremonies of the Scythians, he says,17 "When they have set up three pieces of wood, leaning against each other, they extend round them woollen cloths; and having joined them together as closely as possible, they throw red-hot stones into a vessel placed in the middle of the pieces of wood and the cloths. They have a sort of hemp growing in this country very like flax, except in thickness and height; in this respect the hemp is far superior: it grows both spontaneously and from cultivation; and from it the Thracians make garments very like linen, nor would any one who is not well skilled in such matters distinguish whether they are made of flax or hemp, but a person who has never seen this hemp would think the garment was made of flax. When, therefore, the Scythians have taken some seed of this hemp, they creep under the cloths, and then put the seed on the red-hot stones; but this, being put on, smokes, and produces such a steam, that no Grecian vapour-bath would surpass it. The Scythians, transported with the vapour, shout aloud; and this serves them instead of washing, for they never bathe the body in water."
Mental illusions of all kinds have frequently been looked on as divine revelations, not only by savages, but even by nations having a considerable amount of civilization. The priestess at Delphos became intoxicated with the fumes of narcotic plants before delivering her oracular responses, and it is a curious circumstance that when America was discovered by Columbus, it was the custom of the Indians to throw tobacco on the fire during their religious ceremonies, when the piaches, or priests, who officiated, were thrown into a state of ecstatic inebriation by the smoke they inhaled.
I have already stated my belief that the Indian hemp ad-[11/12] ministered, previous to surgical operations, in China, by Hoa Tho, in the beginning of the third century of our era, was exhibited by inhalation.
The fumes of various narcotic plants are inhaled by eastern nations at present, for smoking in the east is an entirely different process from smoking in the west of Europe, where the fumes of tobacco are merely drawn into the mouth and then puffed out again. In Asia and some of the eastern parts of Europe, the fumes of opium, tobacco, datura, Indian hemp, or whatever else is smoked, are always inhaled into the lungs.
John Baptista Porta of Naples makes the following statement in his work on Natural Magic,18 published in 1597:--
"At last shall be related a wonderful method by which any sleeping person may inhale a soporific medicine. From what we have said, any one will easily know that he is liable to suffer severely after sleep caused by medicine, and to have his suspicions aroused.
"But the quintessence is extracted from a number of the above named medicines by somniferous menstrua. This is put into leaden vessels perfectly closed, lest the least aura should escape, for the medicine would vanish away. When it is used, the cover being removed, it is applied to the nostrils of the sleeping person, he draws in the most subtile power of the vapour by smellings, and so blocks up the fortress of the senses that he is plunged into the most profound sleep, and cannot be roused without the greatest effort. After the sleep, no heaviness of the head remains, nor any suspicion of trick or fraud. These things are plain to the skilful physician, but unintelligible to the wicked."
The author does not make known what the "somniferis menstruis" were, with which the "quinta essentia" were extracted. As sulphuric ether had been described more than fifty [12/13] years before he published his work, it is not improbable that this was the evanescent substance which required to be so carefully closed up, and that the profound sleep was simply caused by this, as the narcotic principles dissolved in it would remain in the bottle in the form of extracts. The benefit of inhalation has been frequently attributed to medicines which were supposed to be inhaled, when it was really due to the menstruum in which the medicines were dissolved. This often happens at present when the menstruum is merely water. Baptista Porta does not say that operations were performed under the influence of the inhalation, or, in fact, that it was applied to any useful purpose whatever.
The Persian Pharmacopœia19 contains some recipes for fumigation, called bouc-houri, that were inhaled, for the medicines are directed to be made up into balls or cubes which are to be placed on the live coals, and the head is to be held over them. Some of the prescriptions contain myrrh, camphor, mace, and storax, and are for the cure of coryza and catarrh; one containing musk, camphor, guaiacum, etc., is said to comfort the brain and intellect, and to be useful in palpitation of the heart, faintness, and debility of the senses. This Pharmacopœia also contains20 a "remėdium odorativum somniferum", which consists of opium and camphor, besides the seeds of roses and the root of mandragora. The ingredients are to be powdered and put in a box, for the purpose of being smelt at. There is also20a a stupifying remedy prepared with five drachms of opium and ten drachms of black poppy, which are directed to be boiled to dryness in water with a pound of wheat, and then powdered. It is added that whoever shall take a drachm and a half of this wheat will be alienated from his senses. With regard [13/14] to the last but one of the above prescriptions--that to be put in a box for smelling, it may be observed that, as heat was not applied, the only ingredient which would produce any effect is the camphor.
The discoveries of Cavendish, Priestley, Lavoisier, and others respecting the nature of atmospheric air and the more important gases, gave an impetus to medicinal inhalations, at the latter part of the last century. Dr. Beddoes, in particular, distinguished himself by the administration of oxygen, hydrogen, carbonic acid, and other gases, in consumption and various diseases. Dr. Richard Pearson exhibited the vapour of ether in consumption with some advantage in the year 1795.21 Three years afterwards, a medical pneumatic institution was established at Bristol, by the exertions of Dr. Beddoes and others. The celebrated Humphrey Davy was the superintendent. This establishment was not very successful in the immediate objects for which it was instituted, but Davy made at this place his masterly researches concerning nitrous oxide gas. In the course of his experiments, he found that severe pain arising from inflammation of his gums was relieved by breathing this gas, and he published the following opinion:--
"As nitrous oxide in its extensive operation seems capable of destroying physical pain, it may probably be used with advantage during surgical operations in which no great effusion of blood takes place."22
This suggestion of Sir Humphrey [sic] Davy was not acted on either by himself or any other person for nearly half a century, when the late Mr. Horace Wells, Surgeon Dentist of Hartford, Connecticut, having witnessed the exhibition of nitrous oxide gas by a public lecturer, named G. Q. Colston, was induced, in consequence of what he saw of its effects, to [14/15] request Mr. Colston to accompany him to his office and exhibit the gas to him, whilst another dentist, named Dr. Riggs, extracted a tooth for him which was troublesome. The tooth was extracted without pain, and Mr. Wells, after the effect of the gas had subsided, exclaimed, "A new era in tooth pulling." This took place on December 11th, 1844.23 Mr. Wells administered the nitrous oxide in thirteen or fourteen cases of tooth drawing in Hartford with a success more or less complete, and before the end of the year he repaired to Boston to introduce his discovery to the professors at the Massachusetts General Hospital. He called on Drs. Warren and Hayward, who invited him to exhibit the gas to one of the patients, who was expecting to have a limb amputated. He remained two or three days in Boston, but the patient decided not to have the operation performed at that time. The nitrous oxide was consequently tried on an individual who required to have a tooth extracted. This patient felt some pain, and the application was considered to be a failure. It is worthy of remark that Drs. Charles T. Jackson, and W. T. G. Morton, were present on this occasion. Mr. Wells returned to Hartford in disappointment. He expressed his opinion to his friends that the nitrous oxide gas was uncertain in its action, and not to be relied on; and he altogether abandoned the use of it until some time after Dr. Morton's discovery of the effects of sulphuric ether in preventing pain.
As long ago as 1818 an article, which is believed to have been written by Mr. Faraday, appeared in the Quarterly Journal of Science and Arts,23a describing the great resemblance between the effects of the vapour of ether and nitrous oxide gas. This circumstance has since been published in all the standard works on chemistry; and it was the annual [15/16] custom of the late Professor Turner, of University College, London, to, pour a little ether into a bladder of air, and allow some of the students to inhale the vapour. The same practice prevailed, more or less, in other colleges, both in Europe and America, when the lecture on ether was delivered. The resemblance between the action of nitrous oxide and that of vapour of ether was therefore extensively known.
Dr. Morton, surgeon dentist of Boston, in America, administered sulphuric ether, by inhalation, to a man in his office, on the 30th of September, 1846, and extracted a tooth without causing any pain. He applied the ether in several cases of a similar kind during the next few days. Having obtained the permission of Dr. J. C. Warren, he administered it to a patient in the Massachusetts General Hospital, on whom that surgeon performed an operation on the neck. On the following day, Dr. Morton exhibited ether to a woman in the same hospital, whilst Dr. Hayward removed a large fatty tumour from the arm, and after this date it was frequently administered.
Dr. Morton was well acquainted with Mr. Horace Wells, before alluded to, and had been in partnership with him. Before administering the ether to his patient in [on] September 30th, Dr. Morton had a conversation with Dr. Charles J. Jackson, Professor of Chemistry, respecting the safety and propriety of the application, and the names of these gentlemen were associated in a patent which they took out for the discovery. Dr. Jackson asserts that Dr. Morton knew nothing of the effects of the vapour of ether till he gave him the information; whilst the latter says it was his intention to use the ether before he went into Dr. Jackson's laboratory. It seems impossible to arrive at the exact truth on this point, but it is admitted on all hands, that Morton was the first who administered ether to prevent [16/17] the pain of an operation. Dr. Jackson23b has indeed claimed the whole merit of the discovery, on the ground of the alleged information he gave to Dr. Morton; but, if every word Dr. Jackson says be admitted, it only appears that he suggested the use of ether to Dr. Morton, just as Sir Humphry Davy had suggested the use of nitrous oxide to all the world in the year 1800. Dr. Jackson had inhaled ether as hundreds of others had done, and being aware of Davy's suggestion of nitrous oxide for preventing the pain of operations, he concluded that ether might also have that effect.
It will be shown further on that Mr. Waldie, of Liverpool, had a greater share in the introduction of chloroform than Dr. Jackson had in the introduction of ether--even supposing that Dr. Morton was previously quite ignorant of that medicine; for when he informed Dr. Simpson of the existence and nature of chloroform, he was able to give him, not merely an opinion, but an almost certain knowledge of its effects; yet Dr. Simpson is justly considered to be the person who discovered and introduced the use of undiluted chloroform as a substitute for ether.
The practice of the ancients in giving mandragora and Indian hemp has no connection with the recent discovery for preventing the pain of operations, which may be briefly related as follows:--Sir Humphry Davy made the suggestion that nitrous oxide gas might be employed for this purpose, and, at the end of forty-four years, Mr. Horace Wells carried this suggestion into practice, but failed to bring the nitrous oxide into general use, and gave the matter up. Two years later, Dr. Morton, who was well acquainted with the efforts of Mr. Wells, applied the vapour of ether, which was already known to resemble nitrous oxide in its action. He succeeded completely in preventing the pain of operations, and [17/18] in bringing his discovery into general use throughout the civilized world. In a short time the inhalation of ether was found to be so safe and certain in its action, and to prevent the pain of operations so entirely, that the most ardent imagination could scarcely conceive that anything further could be desired in this direction.
Dr. Morton withheld at first the name of the agent he was employing, but its strong and peculiar odour revealed it so plainly that concealment was impossible. Dr. Bigelow, of Boston, having tried sulphuric ether, and found it to produce all the effects of the so-called letheon, he made the subject known, not only to his own countrymen, but also by letter to Dr. Boot of London. The first operation under the influence of ether on this side of the Atlantic, was the extraction of a tooth, at the house of Dr. Boot, on Dec. 19th, 1846. Mr. Robinson, of Gower Street, administered the ether and performed the operation. The patient was a lady, named Miss Lonsdale. The ether was quite successful in preventing the pain in this case, as well as in two operations performed at University College two days afterwards, by the late Mr. Liston. These operations were amputation of the thigh, and evulsion on both sides of the great toe nail. The ether was given by Mr. Squire, of Oxford Street, with an apparatus which he contrived for the occasion.
Considerable opposition was made to the inhalation of ether in America, soon after its introduction, and it seemed likely, to fall into disuse, when the news of its successful employment in the operations of Mr. Liston, and others in London, caused the practice of etherization to revive. Mr. Robinson, dentist, gave much time and attention to the exhibition of ether in London on its first introduction, and was on the whole very successful. This was not generally the case, however, with other operators during the first six weeks of the new practice. Owing to imperfections in the [18/19] inhalers employed and in the method of using them, the ether often either failed altogether or only made the patient partly insensible; and Mr. Liston, and some other surgeons, were inclined to discountenance the use of it, in consequence of the struggles and cries of patients to whom it had been administered.
It soon became apparent, however, that the vapour of ether was capable of inducing a state of perfect quietude, with entire absence of pain, during all kinds of surgical operations. From the 28th of January the ether produced the desired effect in every operation that was performed in St. George's Hospital, until the time when chloroform was introduced as a substitute for this agent.24
Ether was employed in Paris a few days after its first application in London, and in a short time it was in use nearly all over the world.
On the 19th of January 1847, just a month after the first application of ether for the prevention of pain on this side of the Atlantic, Dr. Simpson of Edinburgh administered the vapour in a case of labour, and ascertained that it was capable of removing the sufferings of the patient without interfering with the process of parturition. Etherization was soon afterwards employed in the reduction of strangulated hernia and dislocations of the femur and humerus, some of them of long standing. It was also used with advantage in neuralgia, tetanus, and the convulsions of infants, and it became more and more general in surgical operations.
No great improvement in the practice of medicine was probably ever established so readily as the inhalation of ether for the prevention of pain. Yet it met with stout opposition in certain quarters, and when a serious operation [19/20] in which ether had been used terminated unfavourably, there were those who attributed the patient's death to the new practice, although numerous other patients had sunk in exactly the same manner long before ether was used. In one of these cases a coroner's inquest was held, and the jury returned a verdict that the death of the deceased was caused by the inhalation of ether, although the patient had not even been made insensible by it, had felt all the pain of the operation, which was retarded by her struggles, and did not die till the third day. Notwithstanding a certain amount of opposition and mistrust, the inhalation of ether was becoming more general in the course of the year 1847, and there is every reason to conclude that it would very soon have obtained the complete confidence of the medical profession and the public, had it not been for circumstances which must next be considered.
A medicine called chloric ether has been in use since 1831. It consists of a solution of chloroform in spirits of wine. It is somewhat variable in strength, but usually contains about twelve per cent of its volume of chloroform. Dr. Henry Jacob Bigelow of Boston tried this by inhalation, as well as other substances, when Dr. Morton first used sulphuric ether, but he did not succeed with it in causing insensibility to pain. Mr. Jacob Bell of London tried the chloric ether in the beginning of 1847, and succeeded in causing insensibility with it in some cases.25 After this time the chloric ether was exhibited occasionally in St. Bartholomew's and the Middlesex hospitals, and in the private practice of Mr. Lawrence, but it did not come into general use, owing to its expense, and its frequently failing to cause insensibility.
The relation of chloroform to chloric ether is exactly the [20/21] same as that of opium to laudanum, and no one acquainted with this circumstance could doubt for a moment that chloroform inhaled alone would produce the effects which it did when inhaled from its solution in spirit; the only uncertainty about the matter that could possibly exist would be whether it might not be too strong for use in its undiluted state.
The true nature of the so called chloric ether was, however, known to very few persons. It did not enter into the pharmacopœias, and it was mentioned in very few of the works on materia medica. I examined a specimen of it, and found that its properties when inhaled were due to a volatile body containing chlorine, which evaporated first, leaving a great quantity of spirits of wine behind. I concluded that the volatile body was hydrochloric ether, and as this article is so volatile that it exists in the form of gas except in comparatively cold weather, and consequently could not be conveniently used for inhalation, I did not consider the matter any further. M. Flourens had indeed experimented on animals with undiluted chloroform, but was so struck with its great and dangerous power, that he was far from recommending its use in surgical practice.
It was left for Dr. Simpson of Edinburgh, who had already the merit of having discovered the use of inhalation in midwifery, to be the first to administer chloroform in an undiluted state, and to recommend it successfully for general use. Mr. Waldie, of the Apothecaries' Hall of Liverpool, first mentioned chloroform to Dr. Simpson, as the latter states in a foot-note to his first pamphlet on the subject. Mr. Waldie has given the following account of the circumstance in a pamphlet on chloroform.26
"When in Scotland, in October last, Dr. Simpson introduced the subject to me, inquiring if I knew anything likely [21/22] to answer. Chloric ether was mentioned during the conversation; and, being well acquainted with its composition, and with the volatility, agreeable flavour, and medicinal properties of the chloroform, I recommended him to try it, promising to prepare some after my return to Liverpool, and to send it to him. Other engagements and various impediments prevented me from doing this so soon as I should have wished; and in the meantime Dr. Simpson, having procured some in Edinburgh, obtained the results which he communicated to the Medico-Chirurgical Society of Edinburgh on the 10th of November, and which he published in a pamphlet entitled--'Notice of a New Anæsthetic Agent as a Substitute for Sulphuric Ether in Surgery and Midwifery.'"
Dr. Simpson's first experiments with chloroform were made in the early part of November 1847, and his pamphlet on the subject, which was published on the 15th of that month, had a wide circulation, and created great interest. Chloroform was immediately used everywhere to a greater extent than ether had been. An impression became very prevalent that chloroform was safer than ether. This impression arose rather from the general tenour of Dr. Simpson's essay than from any direct statement, for he had not treated on this point.
The great strength of chloroform as compared with ether, and the extreme care required in its use, were indeed soon pointed out;27 these precautions, however, attracted but little attention till the first death from chloroform occurred near Newcastle on the 28th January, 1848. Ether was exhibited by inhalation during eleven months in Europe, and about sixteen months in America, before chloroform was introduced. During all this time no death was occasioned by its use, if we except one at Auxerre in France, [22/23] which appeared to be occasioned by want of air, owing to an imperfect inhaler, and not to the effect of ether. Chloroform had only been employed between two and three months when the above mentioned death occurred, and this was soon followed by others in nearly all parts of the world. These accidents have prevented many persons from inhaling chloroform, and they have prevented a still greater number from enjoying that freedom from anxiety and apprehension before an operation, which ought to be one of the greatest advantages of any plan for preventing pain. As chloroform possesses advantages over ether, in being more convenient and less disagreeable, it continues to be used, to the exclusion of the latter agent, in most parts of the world. In the Massachusetts General Hospital, however, where sulphuric ether was first employed, it was resumed three or four years ago, and the use of chloroform was prohibited by the governors, on account of two accidents from it. Ether is also employed out of the hospital, both in surgical and obstetric practice, in Boston and the neighbourhood; and I have been informed that this is also the case in Philadelphia, whilst in the state of New York both chloroform and ether are employed. I learned last year that ether was the agent employed for causing insensibility at Naples and at Lyons.
Several volatile substances have been tried in a few cases with the effect of causing insensibility, since the introduction of chloroform, but none of them came into use except amylene, which was first employed by me in King's College Hospital in November 1856, after I had made several experiments on animals with it, and inhaled small quantities of it myself. I have administered it in a great number of operations already, and find it to possess certain advantages over chloroform in the greater number of cases. Although it has not yet been generally employed in this country, it [23/24] has been used extensively in Paris, Strasbourg, Lyons, and other places on the continent, with very favourable results.
It is not improbable that, amongst the multitudes of new bodies which chemistry makes known every year, some agent may be found superior to those hitherto used; and besides the great practical advantages which are directly derived from the discovery of inhalation for the prevention of pain, the method of breathing medicinal substances in the gaseous state offers great facilities for the investigation of their effects, and cannot fail to hasten the time when the mode of action of medicines will be a branch of exact knowledge. [24/25]
Inhalation is simply the act of breathing, or at least so much of it as consists of inspiring, or drawing the air into the lungs. The term is usually applied when any medicinal substance is added to the air which the patient breathes, and the process is altogether different from that called "smoking," as practised by the nations of western Europe and of America, where the fumes of tobacco are merely drawn into the mouth and puffed out again. The eastern nations, however, always inhale when they smoke, as was stated before (page 12). This process of inhaling smoke, as I first witnessed it in a gentleman connected with one of the eastern embassies to this metropolis, is very instructive, as showing that the lungs become emptied of their contents by three rather full expirations and inspirations. When this gentleman took the cigar from his mouth to speak, the smoke could be seen issuing thickly with each word till there was a momentary pause as he took a fresh inspiration, then the smoke could be seen issuing with each word as before, only not so thick, and after another inspiration, the smoke could be still perceived in the expired air, but in a very diluted state; but after a third inspiration, it could no longer be seen till he had resumed the cigar.
The following are the chief reasons for resorting to inhalation. [25/26]
1. Certain agents, as nitrous oxide and oxygen, being permanently in the gaseous form, cannot be administered in any other way.
2. By taking advantage of the immense surface of the air cells of the lungs for absorption, a more sudden and profound effect may be produced by medicine than it would be safe, or, in some cases, even possible to produce in any other way. It is to this circumstance, and to the rapidity with which certain volatile medicines exhale in the breath, and leave the patient free from their effects, that the power of preventing the pain of surgical operations is due.
3. Many medicines which have a disagreeable taste--as turpentine, creasote, and camphor--are not unpleasant when inhaled in the form of vapour and the process of digestion is less interfered with than by taking them into the stomach.
4. Medicines, such as benzoic acid, and some of the gum-resins, which are believed to exert a local action on the mucous membrane of the air-passages, may be expected to have a greater effect when inhaled, than when they are taken into the stomach in the same doses, and reach the lungs only through the circulation.
5. Some agents, as chlorine and ammonia, have a local action when inhaled, which they could not exert if exhibited in any other way.
In every kind of inhalation, the breathing should be allowed to go on freely, and in the natural way.
Medicines may be inhaled either at the ordinary temperature, or with the aid of artificial heat and in the latter case they may be breathed with the addition of vapour of water, or with only so much of it as is naturally present in the atmosphere. The medicines in use for the prevention of severe pain, are always inhaled at the ordinary temperature. [26/27]
History and Composition. Chloroform was first made in 1831 by two chemists who operated independently of each other. The liquid, which is formed by the union of equal volumes of chlorine and olefiant gas, and which is usually called Dutch liquid, was named chloric ether by Dr. Thos. Thomson (System of Chemistry, 6th ed., 1820). In consequence of a statement in Silliman's Elements of Chemistry, that the alcoholic solution of this chloric ether was useful in medicine as a diffusible stimulant, Mr. Guthrie, an American chemist, attempted an easy method of obtaining it.28 He distilled together chloride of lime and alcohol, and he considered that the product he had obtained was an alcoholic solution of the chloric ether of Dr. Thomson,28a and it is still used in medicine under that name. About the same time, M. Soubeiran distilled together the above ingredients in France, and analysed the chloroform which he obtained. His analysis, which was incorrect, led him to name the liquid bichloric ether.29 In 1832, Liebig examined the liquid which has been since named chloroform, but as he failed to detect the hydrogen which it contains, he called the liquid chloride of carbon,30 a name which its alcoholic solution occasionally bore afterwards when used as a medicine. In 1834, Dumas examined this liquid. He proved that Soubeiran and Liebig had not obtained it pure, or had been incorrect in their analysis.31 He showed that it consists of two atoms carbon, one atom hydrogen, and three atoms chlorine.
Dumas gave the name of chloroform to the liquid, on [27/28] account of the relation it bears in composition to formic acid, which consists of two atoms carbon, one hydrogen, and three oxygen.32 Liebig, who, in common with other chemists, admits the accuracy of Dumas' analysis, has proposed the name of perchloride of formyle.33 He supposes that the carbon and hydrogen which enter, in the same definite proportion, into numerous compounds, form a base which he calls formyle; and although this base has never been obtained in a separate form, its existence is well supported by analogy, and the term formyle is useful in assisting the memory to retain the composition of a number of substances. For all practical purposes, however, the medicine we are considering is likely to go by the name of chloroform. In the last edition of the London Pharmacopœia, the article has received a name intermediate between the other two. It is called chloroformyl, a name which departs from the brevity of the word chloroform, without having the merit of expressing the chemical constitution of the substance. I believe that no one uses the word chloroformyl; not even the Fellows of the College of Physicians in their individual capacity.
Mode of Preparation. Chloroform can be obtained in various ways, but the most convenient process, and the one which yields it in greatest purity, is that alluded to above, by which it was first procured. The following are the directions in the London Pharmacopœia for making it.
"Take of chlorinated lime, lb. iv [four Troy pounds, or 48 ounces]; rectified spirit, Oss [½ pint]; water, Ox [ten pints]; chloride of calcium, broken in pieces, Ʒj [1 drachm]. Put the lime first mixed with the water into a retort, and add the spirit to them, so that the mixture may fill only the third part of the retort. Then heat them in a sand-bath, [28/29] and as soon as ebullition begins, withdraw the heat as quickly as possible, lest the retort should be broken by the sudden increase of heat. Let the liquid distil into the receiver so long that there may be nothing which subsides, the heat being reapplied if necessary. To the distilled liquid add a quarter of the water, and shake them all well together. Carefully separate the heavier portion which subsides, and add the chloride to it, and frequently shake them for an hour. Lastly, let the liquid distil again from a glass retort into a glass receiver."34
Some manufacturers of chloroform prefer to rectify it from dry carbonate of potassa, since they consider that it is liable to get an acid reaction from decomposition of the chloride of calcium, when it is distilled from that substance. The truth is, however, that there is very little occasion to use either of these substances; for the small quantity of water which chloroform can hold in solution is of no consequence.
Chemical and Physical Properties. Chloroform is a clear colourless liquid, having a hot and intensely sweet taste. It is not inflammable, but when paper moistened with it is introduced into the flame of a candle, it is destroyed with the evolution of smoke and chlorine gas. It is just half as heavy again as distilled water. Its specific gravity was formerly stated to be 1.483, but the liquid used for inhalation of late years has been heavier than this. I find that pure chloroform, when saturated with water, has a specific gravity of 1.500 at 60° Fah.; and after agitating it with sulphuric acid, to deprive it of the water, the specific gravity is 1.503. The amount of water that chloroform can hold in solution is only one part in from 200 to [29/30] 300; and when this is separated by oil of vitriol, the chloroform is liable to undergo spontaneous decomposition.35
Chloroform is soluble in alcohol and ether in all proportions, but it is very sparingly soluble in water. It has been said to require 2000 parts of water for its solution, but this is an error. As the solubility of this and similar medicines in watery fluids has a very important connexion with their physiological action, I took great pains to ascertain the solubility of chloroform correctly. By admitting small quantities of water into graduated jars containing chloroform vapour, I was able to ascertain that chloroform is soluble in about 288 times its volume of water. Chloroform is itself an active solvent of many bodies; dissolving camphor, caoutchouc, gutta percha, wax, resin, iodine, and some other substances very readily. It is a very mobile liquid, and when dropped from the lip of a small phial, the drops are very small. There are three drops to a grain of the liquid, and as a minim of it weighs a grain and a half, there are nine drops in two minims. Consequently persons should not speak indiscriminately of drops and minims, as they sometimes do, when talking of chloroform.
Adulterations. The odour of chloroform is by no means disagreeable. The only liquids that resemble it in smell are Dutch liquid and the chlorinated products of hydrochloric ether, but as they are much more difficult to prepare than chloroform, they are not likely to be substituted for it, or used for its adulteration. The smell of chloroform is therefore a good criterion of its purity and identity. When dropped on the hand, it should quickly evaporate, leaving not the least moisture or smell behind. If a disagreeable odour remains on the hand after the evaporation of the chloroform, it has [30/31] probably been made from impure spirit, or even from wood spirit or acetone, and is unfit for medicinal use.36 When chloroform becomes decomposed from any cause, it acquires a greenish-yellow colour, and gives off chlorine and hydrochloric acid, so that the alteration is at once apparent. When chloroform is pure it has no reaction on test-paper, but is quite neutral. The best way to detect a small quantity of hydrochloric acid in it, is to moisten a slip of blue litmus paper with distilled water, and hold it just within the neck of the bottle exposed to the vapour. If sulphuric acid should be present, it may be discovered by agitating the chloroform with distilled water, and adding nitrate of baryta.
The only article that can be mixed with chloroform without altering its appearance and smell is alcohol. This can be detected by the reduction it occasions in the specific gravity of the chloroform; or, if it be present in any considerable quantity, it may be discovered by adding water to a little of the chloroform in a graduated tube or measure, when a diminution of its volume takes place, owing to the water abstracting the alcohol. The chloroform also acquires a milky opacity under these circumstances. M. Miahle37 speaks of the milky opacity of the chloroform on the addition of water as a very delicate test of the presence of alcohol; but I find that it requires upwards of two per cent of alcohol to cause this appearance on the addition of water.
It has been asserted, and often repeated, that the presence of alcohol in chloroform causes it to have caustic properties, and makes its vapour unusually irritating. I have never seen any evidence of this, although I have had hundreds of [31/32] opportunities of witnessing the action of chloroform mixed with spirit. Under certain circumstances, it is advisable to dilute chloroform with alcohol previous to its administration, as will be explained hereafter.
The chloroform I have met with in London has always been sufficiently pure for inhalation, except in a few cases where a small quantity had become decomposed, probably from having been left a long time exposed to strong daylight. In these instances, its altered appearance generally prevented its being used. I am not aware of serious consequences having arisen anywhere from the impurity or adulteration of chloroform. A case occurred in the London Hospital, where cough and a feeling of suffocation were caused by hydrochloric acid with which the chloroform was contaminated, but the inhalation was discontinued, and no ill consequences resulted.38
Chloroform should be kept in well-stoppered bottles, and protected from the light. It boils at 140° Fah. under the ordinary pressure of the atmosphere. It is consequently one of the most volatile liquids employed in medicine, with the exception of sulphuric ether and amylene.
The Vapour of Chloroform is more than four times as heavy as atmospheric air. It has a specific gravity of 4.2 at 60° Fah. Under ordinary circumstances, the vapour of chloroform has of course no separate existence, but is always mixed with air. It can exist in a pure state only when the temperature is raised to 140° or upwards; or when the pressure of the atmosphere is in a great measure removed by the air-pump. The quantity of vapour of chloroform that the air will hold in solution at different temperatures, under the ordinary pressure of the atmosphere, depends on the elastic force of the vapour at these temperatures. It is governed by a law precisely analogous to that which [32/33] determines the amount of watery vapour which air will hold in solution.
The following table shows the result of experiments I made to determine the quantity of vapour of chloroform that 100 cubic inches of air will take up, and retain in solution, at various temperatures.
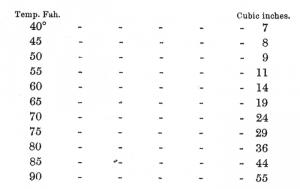
In the above table, the air is a constant quantity of 100 cubic inches which becomes expanded to 107, and so on but it may be convenient to be able to view at a glance the quantity of vapour in 100 cubic inches of the saturated mixture of vapour and air, at different temperatures; and in the table which follows the figures are so arranged as to show this.
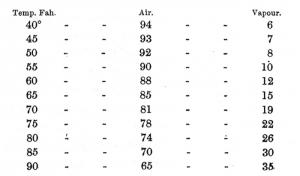
As the effects of chloroform when inhaled depend en-[33/34]tirely on the quantity of vapour present in the air which the patient breathes, the effect of temperature on its volatility is of great practical importance. The air, it is true, does not become fully saturated with vapour during the process of inhalation, but the effects of temperature are relatively as great. If, for instance, a person inhales chloroform from a handkerchief or an inhaler, in such a way that the air he breathes shall be half-saturated with the vapour, then supposing the temperature of the apartment, the handkerchief, etc., to be 50°, the air he breathes will contain 4 per cent; but if the temperature be 70°, the air will contain 9.5 per cent of the vapour.
A considerable amount of caloric becomes latent during the evaporation of chloroform, and the temperature of the vapour and air which the patient breathes are generally reduced a good deal, but not to the same extent as during the inhalation of ether. In giving chloroform from a small sponge which had been squeezed out of water, I have sometimes observed, after laying it down, that it became covered with a kind of hoar frost; the minute particles of frozen water having a slight taste of chloroform. The cold produced by the evaporation of a liquid like chloroform is often the means of checking the evaporation to a certain extent, and limiting the amount of vapour which is taken up by the air.
Chloroform belongs to the large class of medicines known as narcotico-irritants. This and some other agents which have been inhaled for the prevention of pain are often called anæsthetics; a name to which there is no objection, so long as it does not lead to the idea that they have a different action from other narcotics, or more precisely speaking, narcotico-irritants; there being no such medicines as pure [34/35] narcotics. The term anæsthesia has been frequently employed to designate the insensibility and suspension of consciousness caused by chloroform and ether; but, in describing the effects of these agents, I shall confine this term to its original meaning, privation of feeling, and I shall employ the term narcotism to designate the entire effects of these agents on the nervous system. This is the sense in which the term narcotism has always been employed. It has been the custom, however, to restrict the use of the word very much to cases in which stupor existed, but I shall apply it to designate the slighter, as well as the more profound effects of a narcotic, as I am entitled to do by strict etymology.
In order to facilitate the description of the effects of chloroform, I have been in the habit of dividing them into degrees. I use the term degree in preference to stage, as, in administering chloroform, the slighter degrees of narcotism occur in the later stages of the process, during the recovery of the patient, as well as in the beginning. The division into degrees is made according to symptoms, which, I believe, depend entirely on the state of the nervous centres, and not according to the amount of anæsthesia, which there is good reason to conclude, depends, in a great measure, on the local action of the chloroform on the nerves. The different degrees of narcotism glide insensibly into each other.
In the first degree, I include all the effects of chloroform that exist while the patient retains a perfect consciousness of where he is, and what is occurring around him. This degree constitutes all that a person remembers of the effects of the vapour, except when he happens to dream, and recollect it afterwards. The sensations caused by inhaling chloroform are usually agreeable, when it is taken merely for curiosity; and individuals who have inhaled nitrous oxide [35/36] at some previous time of their lives, often describe their feelings as being very much the same from both agents. Patients who are about to undergo a surgical operation are, however, not always in a state for receiving agreeable impressions, and they sometimes complain of palpitation of the heart, and a feeling of fulness in the head. There is generally a sense of dizziness, with singing in the ears and tingling in the limbs. Many persons have a feeling like that of rapid travelling, and as an appearance of darkness sometimes comes on from the failure of the sight, whilst there is also a loud noise in the ears, it not unfrequently happens that a person feels as if he were entering a railway tunnel, just when he is becoming unconscious.
Those persons whose mental faculties are most cultivated appear usually to retain their consciousness longest whilst inhaling chloroform; and, on the other hand, certain navigators and other labourers, whom one occasionally meets with in the hospital, having the smallest possible amount of intelligence, often lose their consciousness, and get into a riotous drunken condition, almost as soon as they have begun to inhale. There is a widely different class of persons who also yield up their consciousness very readily, and get very soon into a dreaming condition when inhaling chloroform. I allude to hysterical females.
There is often a considerable diminution of the common sensibility during the first degree of narcotism by chloroform, more especially when it is inhaled very slowly, so that the patient is kept some minutes partially under its influence. In this way neuralgia can often be relieved, without removing the consciousness, when it is not extremely severe, and the suffering of labour may often be removed in the same manner, when the pains are not very sharp. In a few cases, the extraction of a tooth and other minor operations have been performed without pain, whilst [36/37] consciousness has been retained; but as a general rule, it is better not to operate under these circumstances, for failure is more likely than success; and this plan does not succeed in any case without inhaling longer, and consuming more chloroform, than would be necessary in the usual way. The complete recovery of the patient from the effects of the vapour, after a protracted inhalation of this kind, is also more tardy.
The first degree of narcotism recurs when consciousness returns as the effect of the choloform is subsiding. At this time, there is generally a greater amount of anæsthesia than at the commencement of inhalation, just before consciousness is removed. I have many times known the introduction of sutures, and such like measures, performed at the concluding part of an operation, after the patient had recovered his consciousness, without his feeling what was being done. As a general rule also, the smarting of the wound does not commence till some time after consciousness has returned.
In the second degree of narcotism, there is no longer correct consciousness. The mental functions are impaired, but not necessarily suspended. When a patient inhales chloroform quietly for a medical or surgical purpose, he usually appears as if asleep in this degree; but if his eyelid be raised, he will move his eyes in a voluntary manner. There are occasionally voluntary movements of the limbs; and although the patient is generally silent, he may nevertheless laugh, talk, or sing. Persons sometimes remember what occurs whilst they are in this state, but generally they do not. Any dreams that the patient has, occur whilst he is in this degree, or just going into, or emerging from it, as I have satisfied myself by comparing the expressions of patients with what they have related afterwards. There is sometimes a little trouble with the patient in this degree of [37/38] narcotism. He feels the inconvenience of the vapour he is breathing, and having become unconscious of the object for which it is inhaled, he endeavours to push away the inhaler. As a person in this condition can generally hear and partly understand what is said, a few kind words will often render him tractable. This is generally true of all those who have been brought up with care and kindness, more especially patients of the female sex; but the man who has been roughly treated from the time of his birth, can often be made insensible only by means of a little restraint.
There is generally a considerable amount of anæsthesia connected with this degree of narcotism, and I believe that it is scarcely ever necessary to proceed beyond it in obstetric practice, not even in artificial delivery, unless for the purpose of arresting powerful uterine action, in order to facilitate turning the fœtus. The loss of sensation is indeed sometimes so complete in this degree, especially in children, that the surgeon's knife may be used without pain; I have indeed seen a child unconsciously handling its toys all the time that the operation of lithotomy was performed on it. Commonly, however, the use of the knife, when the narcotism has not proceeded further than this degree, occasions expressions indicative of pain, which are either not remembered, or are recollected as having occurred in a dream. The patient is generally in this degree during the greater part of the time occupied in protracted operations; for although, in most cases, it is necessary to induce a further amount of narcotism before the operation is commenced, it is not usually necessary to maintain it at a point beyond this.
In the third degree of narcotism, there are no longer any voluntary motions. The eyes, for instance, are not directed towards any object; and although the limbs may move, they are not directed to any purpose. The pupils are ge-[38/39]nerally inclined upwards in this degree, and are at the same time usually somewhat contracted. The bloodvessels of the conjunctiva are generally somewhat enlarged in this degree in all persons who are well nourished and not deficient in blood. It is in this degree of narcotism that rigidity and spasms of the muscles occur in certain cases. These phenomena occur most frequently in cases where the muscles have been much exercised, and are consequently well nourished. They are never met with in infancy, and rarely before puberty. They are much more common in the male than the female sex. The rigidity and spasm are greatest and most constant in labourers and persons accustomed to athletic exercises, and they are usually absent in patients who have been long confined to the room, or are much reduced in strength from any cause. They are less marked in old age than in the middle period of life, and they are not by any means so frequent or strong in fat, as in thin, muscular persons. I have seen the spasms take an epileptiform character in a few cases; but by gently continuing the chloroform, they have always been subdued. In a great number of cases, the patient mutters in an almost inarticulate and a perfectly unintelligible manner, just as the muscular rigidity and spasm are subdued. Under these circumstances, I have never heard a single word pronounced so that it could be understood. If articulate language is uttered just after the muscular rigidity, it is evidence that the effects of the chloroform are being allowed to diminish, and that the patient is going back into the second decree of narcotism.
In the third degree of narcotism, a person is quite incapable of having any perception or consciousness of pain, but anæsthesia is not a necessary part of this amount of narcotism when it is first induced, and in some cases a patient may flinch, and put on an expression of countenance which seems indicative of pain. He may also cry out, but not in [39/40] an articulate manner. By continuing the chloroform gently for a minute or so, a state of complete anæsthesia can be induced in nearly every case, without carrying the narcotism of the nervous centres further than this degree. The loss of sensibility of the conjunctiva, as shown by the absence of winking when the edges of the eyelids are gently touched, is the best criterion that the patient will bear the knife without flinching or crying.
The circumstance of the anæsthesia, or loss of common sensibility, not keeping pace with the degree of narcotism of the brain, as shown by the presence or absence of consciousness and volition, appears to depend on the chloroform acting on the peripheral distribution of the nerves, as well as on the nervous centres.39 The following considerations support this view. 1. Chloroform has the effect of diminishing the sensibility of a part to which it is applied locally, even to the sound cuticle. When the cuticle is removed, the local anæsthesia of the surface is complete; and in frogs, which have a thin permeable skin, and a languid circulation, one limb can be rendered insensible, by the local application of this agent, before the remainder of the animal is much affected. 2. Chloroform when inhaled immediately circulates throughout the body, in all parts of which it can be detected by chemical means. 3. Chloroform and other narcotics suspend the function of the nerves, when locally applied to them. 4. When inhaled, the local effect of chloroform must be greatest when it has had time to exude through the coats of the vessels, into the extra vascular liquor sanguinis, and come into immediate contact with the nervous fibrillæ; and it must take some little time after the chief part of the chloroform has escaped from the blood during its passage through the lungs, before that which is in the lymph external to the vessels can pass back [40/41] again into them, by endosmosis. The brain, on the other hand, is without lymph and lymphatics. The blood in this organ is all contained within the vessels, in which, moreover, it circulates with more velocity than in the external parts of the body. It can be easily understood, therefore, how the brain may escape from the effects of the vapour whilst the nerves of sensation throughout the body still remain partially under its influence. 5. It is in young subjects, in whom, connected with the more active process of nutrition, the quantity of lymph external to the vessels is greatest, that the general insensibility most frequently remains, whilst the cerebral hemispheres are resuming their functions; whilst in persons of spare habit, approaching the middle or later periods of life, there is little anæsthesia except in the unconscious state.
The co-operation of the brain with the nerves is, of course, necessary to sensation; and it is possible by a large dose of chloroform to produce complete anæsthesia very suddenly, before there is time for the nerves to be acted on locally to any extent; and if the chloroform is not continued, the anæsthesia may subside as quickly as it was induced. The large ganglia of sensation, the optic thalami, seem to require a greater quantity of chloroform to suspend their function than is necessary to suspend that of the cerebral hemispheres, but, by occupying three or four minutes in giving chloroform, one is enabled to add its local action on the nerves to its influence on the brain, and thus to induce anæsthesia with less narcotism of the nervous centres than would otherwise be required.
It must not be supposed that the difference of the action of chloroform on the cerebral hemispheres, and on the optic thalami, will of itself explain the want of uniformity between the loss of consciousness and loss of feeling. If it were a mere difference of degree, it might be so explained; but the [41/42] absence of all regular relation between these phenomena can only be satisfactorily accounted for when the circumstances connected with the circulation and the liquor sanguinis, that I have endeavoured to explain above, are taken into account.
In the fourth degree of narcotism, the breathing is stertorous, the pupils are dilated, and the muscles completely relaxed. The patient is always perfectly insensible. It is very seldom necessary to carry the effects of chloroform as far as this degree. It is, however, sometimes requisite to do so, in attempting to reduce dislocations of long standing in muscular persons, and whilst the surgeon is dissecting in the neighbourhood of important vessels and nerves, in certain robust subjects and others who seem to have acquired an excess of sensibility by hard drinking, and who can hardly be kept quiet under the knife, except when the breathing is stertorous.
There are some further effects of chloroform with which one becomes acquainted in experiments on the lower animals. If the inhalation is continued after the symptoms just described are produced, the breathing is rendered difficult, feeble, or irregular, and is sometimes performed only by the diaphragm, whilst the intercostal muscles are paralysed. If the dose of chloroform is gradually increased after these effects are produced, the breathing entirely ceases, but the heart continues to pulsate very distinctly, till its action becomes arrested by the absence of respiration, as in asphyxia. This interval, including the embarrassment and cessation of the breathing, I call the fifth degree of narcotism.
Although the respiration may be suspended by an amount of chloroform that has very little direct effect in the motion of the heart, it is quite possible to stop the heart's action by the immediate effect of this agent. When frogs are exposed [42/43] to the action of the vapour, they go on absorbing it by the skin, after the respiratory movements have ceased; and in this way the pulsations of the heart are arrested, when a certain amount of chloroform has been absorbed into the blood. And when animals of warm blood are made to breathe air containing as much as eight or ten per cent of the vapour of chloroform, the blood which is passing through the lungs becomes so charged with it as to stop the action of the heart, when it reaches that organ through the coronary arteries. It is in this way that accidents from chloroform have happened. The power of this agent to arrest the pulsations of the heart can also be shewn, by blowing a stream of the vapour on its surface, when the chest is opened immediately after the breathing has ceased, and whilst it is still beating.
The ultimate and greatest effect that chloroform is capable of producing on the animal body is to destroy the irritability of the muscles, and produce the post mortem rigidity. Either the whole body or a single limb can be rendered instantly rigid by injecting the arteries with a little chloroform shaken up with water. The rigidity remains for weeks in the dead body, and would probably be permanent if the chloroform were prevented from evaporating. Whilst it lasts, putrefaction is of course prevented.
Effect of Chloroform on the Pulse. I have not mentioned the state of the pulse in the above description of the effects of chloroform, for it affords no criterion of the amount of narcotism, and it was better therefore to reserve it for a separate notice. It is nearly always increased both in force and frequency, more especially at the early part of the inhalation. After the patient has become quite insensible, the pulse indeed generally settles down nearly to the natural standard, and in the middle of the most formidable operations, it is often beating with natural volume and force, not [43/44] more than sixty or seventy times a minute. The pulse rarely becomes weaker or slower than natural under the influence of chloroform, except from considerable loss of blood, or where the patient is about to be sick. I have twice found the pulse as slow as 44 in the minute at the conclusion of an operation attended with great loss of blood. One of the cases was the removal of a large tumour of the labium pudendi, in a woman, aged forty-five, on the 28th of April, 1849, at King's College Hospital, by Mr. Fergusson. The pulse was, however, not small or weak, and there was no faintness. In a few minutes, the patient vomited, and the pulse immediately resumed its natural frequency.40
There is occasionally a feeble state of pulse with a feeling of faintness as the effects of the chloroform subside, and in two or three cases in which the patient was in a sitting posture, positive syncope occurred, which, however, was promptly removed by the horizontal position. The persons most liable to a feeling of faintness after chloroform, are those who are subject to syncope from slight causes.
Action of Chloroform on the Nervous System. Chloroform, when inhaled, immediately reaches every part of the nervous system through the circulation, and it acts on every part of that system from the first, as a careful observation of the symptoms proves. It does not, however, act equally on all parts of the nervous system, according to the quantity which is absorbed; some parts of that system have their functions entirely, or almost, suspended, whilst others are but little under the influence of the vapour, and [44/45] it is owing to this fact that the most severe pain may be prevented without danger. M. Flourens made the following remarks respecting the action of sulphuric ether, and they apply equally well to the effects of chloroform, when it is inhaled gradually: "Under the action of ether, the nervous centres lose their powers in regular succession--first, the cerebral lobes lose theirs, viz., the intellect; next, the cerebellum loses its, viz., the power of regulating locomotion; thirdly, the spinal marrow loses the principle of sensitiveness and of motion; the medulla oblongata still retains its functions, and the animal continues to live: with loss of power in the medulla oblongata, life is lost."41 I may add, that after the breathing has ceased, from the loss of power of the medulla oblongata, the ganglionic nerves still perform their functions, and the heart and intestines continue to move for a time, often with vigour.
Owing to the unequal effects of a given quantity of chloroform on different parts of the nervous centres, and owing to its acting also on the nerves, a variety of states may be met with during a surgical operation, some of which have often been thought curious, or anomalous. The most usual state of the patient during an operation, when chloroform is successfully administered, is one of perfect quietude, without any sign of consciousness or sensation. The patient under chloroform may, however, moan, or cry, or flinch, or show other symptoms which are usually thought indicative of pain, but without using any articulate language, or remembering anything of the operation afterwards. If his flinching or crying out has neither interfered with the surgeon, nor distressed the friends who may be present, a case of this kind may be considered satisfactory. A third condition of the patient under the influence of chloroform is that in which he talks, or laughs, or sings during the opera-[45/46]tion, his words having no reference to what is being done. If he is sufficiently quiet for the proceedings of the surgeon, the application of the chloroform must be considered successful, and this condition proves the absence of pain even more completely than that in which there is neither sign nor sound, except the breathing and pulsation of the heart and blood vessels. A fourth condition of the patient is that in which he is conscious, and can look on whilst the surgeon is performing some small operation, or the minor part of a large one, without feeling it, or whilst feeling it in a manner which is not painful. This condition, when it occurs, is the most satisfactory proof of the power of chloroform to prevent pain. It happens but rarely, however, and cannot be induced at will, and it is usually at the concluding part of an operation, during which the patient has been unconscious, that this condition is met with. He wakes whilst there is still a vessel to tie, or a suture to be introduced, and does not feel it, owing, as was stated before, to some of the chloroform being detained in the extra vascular liquor sanguinis, whilst the brain has become almost free from the medicine. When the knife, or the needle, is felt without being painful, it is because the common sensibility, without being entirely abolished, is so much reduced, that what would otherwise cause acute pain only occasions an ordinary sensation.
A fifth state of the patient is met with when an insufficient quantity of chloroform has been administered, or when its effects have been allowed to subside too soon. The patient may call out or complain in articulate words, such as "Oh, you are hurting me," and yet may assert afterwards that he had no pain, and knew nothing whatever of the operation. His own language at the time must, however, be held to decide that there was some pain, which made so slight an impression on the disordered mind as not [46/47] to remain in the memory. Pain which is not remembered is of very little consequence, and probably is but slight in degree. It should not be judged of by the expressions of the patient when he is but partially conscious, and using no self-control. Chloroform may, lastly, be administered so badly, that the patient simply falls asleep under the soothing influence of a very gentle dose, as he might sleep from an ordinary dose of opium, without being insensible, and, when the operation is commenced he wakes to full consciousness, and both feels pain and remembers it.
Patients, when insensible, sometimes moan or groan from the effects of the chloroform, and quite independently of the operation. The groaning or moaning comes on sometimes and even leaves off again, before the operation is commenced. When symptoms like those of pain are present during an operation, one may generally know whether they are the consequences of it, by observing whether or not they are connected with each cut of the knife. But even when a flinch or a groan follows each manipulation of the surgeon, it does not necessarily follow, provided the patient does not speak, that he is suffering pain. Some amount of consciousness is essential to the presence of pain, but many of the lower animals execute movements like those caused by pain, after the head is cut off, and when, of course, there can be no consciousness. Although the mind, under ordinary circumstances, is conscious of the attitude, gestures, and cries, which accompany pain, neither the intellect nor the will have any share in their production. On the contrary, they usually take place in spite of the efforts of the will to prevent them, and one may understand that, when consciousness and volition are suspended, the actions usually indicative of pain may, for want of control, be excited by slighter causes, and to a greater degree, than in the waking state. [47/48]
It is certain that chloroform may prevent pain in two ways, either by rendering the mind unconscious of external impressions, or by removing the sensibility to these impressions, that is, by a true anæsthetic action, but usually, and always when breathed in a full dose, it acts in both ways at once.
The patient sometimes supposes that he remembers all the particulars of the operation, although he did not feel the pain, but on questioning him it is usually found that it is a dream which he remembers, and not the actual facts. It is extremely rare for a patient to assert that he has felt pain from the operation, when he has not felt it, but I have known this to happen once or twice, and a circumstance which was related to me by Mr. Robinson proves the possibility of it. He administered chloroform, or ether, to a lady, with the intention of extracting some teeth, but could not succeed in getting the mouth open, and the lady woke before anything had been done, and asserted that she had felt the operation. She inhaled again, and awoke, and repeated the same statement once or twice before the teeth were actually extracted.
I have heard it stated that patients have felt the pain of the operation, but have been unable to make any sign of feeling it. Such an occurrence may possibly take place when the chloroform is inhaled too slowly, or not in sufficient quantity; but I have not witnessed it, and it evidently cannot happen with a sufficient dose.
I arrived at the conclusion, after much careful observation, that chloroform might be given with safety and advantage in every case in which the patient requires, and is in a condition to undergo, a surgical operation; and having [48/49] acted on this conclusion for several years, I have found no reason to change it. It is desirable, however, to pay attention to every circumstance connected with the health and constitution of the patient before exhibiting chloroform, as many of these circumstances influence its effects.
Age. The age of the patient has considerable influence in modifying the effects of chloroform. It acts very favourably on children: they sometimes oppose the inhalation of it as long as they are conscious, but it does not occasion the rigidity and struggling after loss of consciousness, which are sometimes met with in the adult. Anæsthesia is generally induced with a less amount of narcotism of the nervous centres in children than in grown up persons. The effects of chloroform are more quickly produced and also subside more quickly in children than in adults, owing no doubt to the quicker breathing and circulation. It often happens, however, that when the insensibility has been kept up for some time, say twenty minutes or half an hour, in a child, it is followed by a natural sleep of a few hours duration, provided there is no painful wound, or other cause, to prevent the sleep. I have given chloroform in a few cases as early as the ages of eight and ten days, and in a considerable number before the age of two months; and I have at this time, June 30th, 1857, memoranda of the cases of 186 infants under a year old to whom I have administered this agent. There have been no ill effects from it either in these cases, or in those of children more advanced in life; and it is worthy of remark that none of the accidents from chloroform which have been recorded, have occurred to young children.
There is nothing peculiar in the effects of chloroform on people advanced in years, except that its influence subsides rather slowly, on account of the slower breathing and circulation. I have given chloroform to many patients over [49/50] seventy-five years of age, and to one as old as ninety years.
Strength or Debility. The comparative strength or debility of the patient has considerable influence on the way in which chloroform acts. Usually the more feeble the patient is, whether from illness, or any other cause, the more quietly does he become insensible; whilst if he is strong and robust, there is very likely to be mental excitement in the second degree, and rigidity of the muscles, and probably struggling in the third degree of narcotism. Patients in a state of debility resemble children, not only in coming quietly and easily under the influence of chloroform, but also in the circumstance, that the common sensibility is suspended with less narcotism of the nervous centres than is generally required in robust persons. Children and persons in a state of debility have usually an acute sensibility which causes them to suffer pain from very slight injuries, but this sensibility is more easily suspended by chloroform than the less acute sensibility of robust persons. It is in strong men, accustomed to hard work or athletic sports, that the rigidity and struggling previously alluded to in describing the effects of chloroform, most frequently occur after the loss of consciousness. Some of the patients in whom the struggling and rigidity have been greatest were gentlemen belonging to boating clubs; but I think the patient, in whom these symptoms were most violent, was a celebrated harlequin of one of the London theatres, on whom Mr. Fergusson operated a few years ago.
The persons in whom the rigidity and struggling are well marked are often lean and wiry, and these symptoms rarely occur in fat people. The rigidity and struggling are less marked when the chloroform is given slowly than when quickly given.
Hysteria. Patients who are subject to hysteria sometimes have symptoms of the complaint, such as sobbing, crying, [50/51] or laughing, as soon as consciousness is suspended, or even impaired, by the chloroform; but these symptoms can always be subdued by proceeding with the inhalation. In a very few instances the hysterical state returns, and becomes troublesome as the effect of the vapour subsides. In two or three cases that I have met with, it continued for three or four hours, but it usually subsides in a much shorter time. The inhalation should not be suspended on account of the hysteria, but should be continued till it is subdued before an operation is performed.
I have rarely seen a decided fit of hysteria from the effects of chloroform, but in the case of a young married lady, to whom I gave this agent to prevent the pain of an operation on the rectum, a somewhat violent paroxysm of hysteria came on directly after the inhalation was commenced. The surgeon would not permit me to continue the chloroform, and expressed his intention of operating without it. After waiting for about half an hour, however, for the hysteria to subside, and finding that it continued the same as at first, the inhalation was resumed. The patient was soon rendered insensible, and lay perfectly still whilst the operation was performed. There was a little hysteria as the effects of the chloroform subsided, but not so severe as before.
I have several times seen hysterical symptoms in the male, either during the administration of chloroform, or whilst the patient was recovering from its effects. But in all these cases, the patients informed me afterwards that they were subject to hysterics when under the influence of mental emotion.
In some persons who are subject to hysteria, the breathing becomes excessively deep and rapid whilst inhaling chloroform. This usually occurs just as the patient is becoming unconscious, but in a few cases even earlier, and the [51/52] patient is aware of the impulse to breathe in this manner. After this kind of hysterical breathing has lasted a minute, the patient is aware of the impulse to breathe in this manner. After this kind of hysterical breathing has lasted a minute, the patient generally rests nearly a minute without breathing at all, after which the respiration generally becomes nearly natural. I give the chloroform very sparingly during this violent breathing, or else withdraw it altogether for a minute or two.
I do not consider that the hysterical diathesis forms any objection to the use of chloroform in operations, as the patients would be generally quite as liable to suffer an attack of hysteria from the pain, if chloroform were not used.
Epilepsy. Chloroform occasionally brings on a fit of epilepsy in persons who are subject to this disease. It was stated in one of the foreign medical journals, in 1848, that this agent was so certain to cause a fit in epileptic persons, that it might be used to detect impostors pretending to be subject to this disease; but if this assertion has been acted on, it must have led to great injustice, for I have many times administered chloroform to the extent of causing complete insensibility in epileptic patients who required to undergo operations, without its inducing the least approach to a fit.
In the few cases in which epileptic convulsions are occasioned by chloroform, they do not appear till the third degree of narcotism is induced, in this respect differing from hysteria, which comes on in the second degree, or even earlier, as was stated above. The course to pursue, when epileptic convulsions appear, is to continue the chloroform steadily and gently, till they subside. I have never seen the chloroform fail to subdue the convulsions in a very few minutes, and I have never seen them recur after the operation, as the effects of the vapour subsided. In medical and obstetric practice, and for slight operations, it is not requisite to carry the effects of chloroform so far as that stage in [52/53] which an epileptic fit would occur, so that under these circumstances the fact of a patient being subject to epilepsy hardly requires to be taken into account.
Pregnancy. I have repeatedly given chloroform at all periods of pregnancy, both for tooth drawing and more important operations, and I have not met with any ill effects from it in any of the cases.
The Menstrual Period. It is customary to avoid the menstrual period in fixing the time for a surgical operation, when it can be so arranged. There are, however, often reasons for not waiting over this period, and under such circumstances, I do not know any objection to the inhalation of chloroform. I have administered it frequently during the menstrual period, and have seen no ill effects from it. I have observed that there is a little more tendency to slight hysterical symptoms, during its inhalation at this period, than when the same patients inhale it at other times, which is what we might expect.
Diseases of the Lungs. Affections of the lungs sometimes cause a little difficulty and delay in the administration of chloroform, as the vapour is liable to excite coughing when the mucous membrane of the air passages is irritable. The inconvenience is, however, confined to the time of inhalation, for the cough is generally relieved afterwards. I have given chloroform for surgical operations in many cases where phthisis was present, and in several patients who had suffered from hæmoptysis, and have not seen any ill effects from its use in these cases. Chloroform has indeed often been inhaled with advantage to relieve the cough in consumption. The cases of chronic bronchitis in which chloroform is administered for surgical operations are still more numerous. The effects I have observed have been coughing at the time of inhalation, and very often a relief of the cough afterwards. Some of the patients had emphy-[53/54]sema of the lungs. It is scarcely necessary to allude, in this place, to acute diseases of the lungs, as surgical operations are not performed during their continuance, but from the fact of chloroform being inhaled occasionally in the treatment of these affections, it is evident that they would cause no obstacle to its employment.
Disease of the Heart. There is a very general impression that the use of chloroform is unsafe when disease of the heart exists, more particularly, fatty degeneration of that organ. This belief has been encouraged by the circumstance that this affection has been present in a few of both the real and alleged deaths from chloroform; and also by the fact that, in the accidents that have been really due to chloroform, the heart has been the organ on which it has exerted its fatal influence. When we come to investigate these cases, however, we shall find reason to conclude that the heart has probably been diseased in quite as great a proportion of the patients who have taken chloroform without ill effects, as in those who have succumbed under its influence. As regards my own practice, indeed, the only case in which death could in any degree be attributed to the chloroform, was one in which there was extreme fatty degeneration of the heart; but, on the other hand, I have given chloroform in numerous cases without ill effects where the symptoms of this, as well as other affections of the heart, were present in a very marked degree. Indeed, I have never declined to give chloroform to a patient requiring a surgical operation, whatever might be his condition, as I early arrived at the conclusion that this agent, when carefully administered, causes less disturbance of the heart and circulation than does severe pain. Whenever I have had an opportunity of seeing an operation performed without chloroform, I have carefully observed the pulse, and although none of these operations have been of a very severe nature, [54/55] I have found the circulation to be much more disturbed than it would have been by chloroform carefully administered. The pulse in most of these cases has been excessively frequent during the operation, and in some instances it has intermitted to an unusual extent.
In one instance, I had an opportunity of witnessing a similar operation on the same patient, first without chloroform, and afterwards under the influence of this agent. On January the 6th, 1855, Mr. Fergusson performed lithotrity, in King's College Hospital, on a man, aged fifty-one. He generally directs chloroform to be administered in lithotrity, but in this instance he omitted to do so, as he thought that the bladder was not very irritable, and that the patient would not suffer much. I began to feel the pulse just when the patient saw the lithotrite about to be introduced. It was 120 in the minute. As soon as the instrument was introduced, the pulse increased to 144, and immediately afterwards it became uneven, irregular, and intermitting. I could not count more than three or four beats at a time; and, occasionally, when the pain seemed greatest, and the man was straining and holding his breath, the pulse was altogether absent for four or five seconds. In order to ascertain whether the absence of pulse at the wrist might not depend on the pressure of the muscles of the arms, caused by grasping the table, I applied my ear to the chest, and found that there was no sound whatever to be heard during the intervals when the pulse was imperceptible. It was evident that the patient held his breath till the right cavities of the heart became so distended as to stop the action of that organ till the respiration returned. The man did not complain or cry out during the operation. A week afterwards the lithotrity was repeated, but on this occasion I administered chloroform. The pulse was about 120 in the minute when the patient began to inhale the chloroform, [55/56] but it became slower as he was made unconscious, and it was regular and natural during the operation. It was only towards the end of the operation, when the effect of the chloroform was allowed to diminish, and when the man began to strain a little, though not yet conscious, that the pulse intermitted slightly, passing over a single beat occasionally. There were none of the long intermissions of the pulse observed on the former occasion.
It is very evident that if the above-mentioned patient had been the subject of any affection of the heart which weakened or embarrassed its action, he would have run a much greater risk from the pain of the first operation, than from the inhalation of chloroform in the second one.
In a few of the patients having the arcus senilis of the cornea, a weak, intermitting, or irregular pulse, and other signs of fatty degeneration of the heart, there have been a feeling of faintness and a tendency to syncope, as the effects of the chloroform were subsiding, especially when the operation had been performed in the sitting posture; but these symptoms have soon subsided, in all the cases I have met with, on placing the patient horizontally, with or without the help of a little ammonia to the nostrils.
Cerebral Disease. Affections of the head offer no obstacle to the administration of chloroform. I have given it to several patients who had suffered previously from an attack of apoplexy. Some of them still retained the paralysis resulting from their attack, but the chloroform has not been attended or followed by ill effects in any of these cases. The following case, in which alarming head symptoms had existed a few hours before the inhalation of chloroform, cannot fail to be interesting.
The 31st of October, 1854, was appointed by Mr. Fergusson to perform lithotrity on a gentleman, seventy-eight years of age, who had a phosphatic calculus in his bladder. [56/57]He was a patient of Mr. Propert, and Mr. Fergusson had removed a similar calculus by lithotrity, and I had given him chloroform at each of the operations, and it was arranged that he should have chloroform on the present occasion. Mr. Propert informed Mr. Fergusson and me, on our arrival, that his patient had had an attack the night before resembling apoplexy; he had been insensible, the breathing had been stertorous, the pupils dilated, and the face very red and congested. Mr. Propert had caused him to be cupped to fourteen ounces, and had given him twenty grains of calomel in the course of the night, and in the morning he was as well as usual, and remained so at the time of our visit. We considered the case with Mr. Propert, and as there were reasons for not postponing the operation, it was determined that he should inhale the chloroform rather than be subjected to the pain. The vapour acted very favourably; he recovered his consciousness a few minutes after the operation, and expressed himself as feeling quite well.
Mr. Fergusson crushed another calculus in this patient in March 1855, when I again administered chloroform, and in 1856 I understood that he was free from the complaint.
Insanity. Chloroform acts on insane patients just as it does on others, that is to say, they are made insensible by it, and, when its effects completely subside, it leaves them in the same state of mind as before. Insane people are, however, often so suspicious that they cannot be persuaded to inhale chloroform, and it can only be given to them by force. When once under its influence, however, I have seen teeth extracted, and other operations performed, which it would have been impossible to accomplish in the same individuals without resorting to inhalation. The use of chloroform in the treatment of mania will be alluded to in another part of this work.
Hard Drinkers. It was at one time alleged that hard [57/58] drinkers of spirituous liquors were not susceptible of the influence of ether or chloroform, and for a long time there remained an impression that these persons were difficult to render insensible. I have always found that hard drinkers were rendered unconscious, and even comatose, by the same amount of ether or chloroform as other persons; but they sometimes have a morbid excess of sensibility in the nerves of common sensation, and do not lie still under the surgeon's knife except when the nervous centres are deeply narcotised, and the breathing almost stertorous. On this account, they sometimes inhale much more chloroform during a protracted operation than other persons.
Before proceeding to describe the mode of administering chloroform, it is desirable to treat of the quantity of it which produces its different effects. Without alluding to the facts and experiments which prove that all narcotics produce their effects by being absorbed into the circulating fluid, and so reaching the nervous system on which they act, it is only necessary to mention the following circumstances to show that this is the case as regards chloroform. In some experiments in which I assisted Dr. Sibson, we found that the vapour of chloroform produced its effects after both the pneumogastric nerves had been divided, exactly the same as before. Chloroform can be detected by means of chemical tests exhaling in the breath of those who have just previously inhaled it. It can also be detected in the urine after inhalation, and very readily in all the tissues of animals that have been killed by it, for several days after death.
The quantity of chloroform in the blood in the different degrees of narcotism might be estimated approximatively [58/59] from the amount used in inhalation, but I devised some experiments in 1848 for ascertaining the quantity with accuracy.42 The experiments were based on the following circumstances.
When air containing vapour is brought in contact with a liquid, as water or serum of blood, absorption of the vapour takes place, and continues till an equilibrium is established; when the quantity of vapour in both the liquid and air, bears the same relative proportion to the quantity which would be required to saturate them at the temperature and pressure to which they are exposed.
This is only what would be expected to occur; but I verified it by numerous experiments in graduated jars over mercury. The intervention of a thin animal membrane may alter the rapidity of absorption, but cannot cause more vapour to be transmitted than the liquid with which it is imbued can dissolve. The temperature of the air in the cells of the lungs and that of the blood circulating over their parietes is the same; and, therefore, when the vapour is too dilute to cause death, and is breathed till no increased effect is produced, the following formula will express the quantity of any substance absorbed:--As the proportion of vapour in the air breathed is to the proportion that the air, or the space occupied by it, would contain if saturated at the temperature of the blood, so is the proportion of vapour absorbed into the blood to the proportion the blood would dissolve.
The manner in which the experiments were performed, was to place a small animal in a glass jar, so large that it formed a capacious apartment for it, and held much more air than it could require in the course of the experiment. The jar was covered with a closely fitting lid, and a carefully weighed portion of chloroform was allowed to diffuse itself through the air of the jar. The experiments were continued [59/60] till the chloroform produced no further effect. I shall pass over a number of tentative experiments, and adduce only a few of those which were made after I had ascertained the quantities requisite to produce the desired effect. The results obtained in these experiments were entirely due to the degree of dilution of the vapour; for the quantity of chloroform employed was, in every instance, more than would have killed the animal in a much shorter time than the experiment lasted, if it had been conducted in a smaller jar. It is assumed that the proportions of vapour and air remain unaltered during the experiment; for the quantity absorbed must be limited to what the animal can breathe in the time, which is so small a part of the whole that it may be disregarded.
Experiment 1. A guineapig and a white mouse were placed in a jar holding 3,000 cubic inches, and fifteen grains of chloroform were introduced by a tube in the lid of the jar, which was closed immediately by a screw. The chloroform fell on some blotting paper suspended in the jar, and in a minute or two was converted into vapour and diffused through the air in the jar. The animals were allowed to remain half an hour, and were unaffected by the chloroform, except that they appeared to be a little less brisk than usual, during the first two or three minutes after their removal.
Experiment 2. A guineapig was placed in the same jar, and twenty-two and a half grains of chloroform were introduced in the same manner as before, being three-quarters of a grain to each hundred cubic inches of air. In two or three minutes the chloroform was converted into vapour and diffused through the air in the jar. Six minutes afterwards the guineapig began to stagger, and soon afterwards was unable to keep on its legs. It was kept for half an hour in the jar, but did not become further affected. It was occasionally quiet, but always tried to walk when disturbed by [60/61] moving the jar. When taken out, it flinched on being pricked, and it tried to walk, although unable to support itself on its legs. It recovered from the effects of the chloroform in three or four minutes.
Experiment 3. Another guineapig was placed in the same jar, and thirty grains of chloroform were introduced. In three or four minutes the chloroform had evaporated and diffused itself through the air in the jar. In two minutes afterwards the guineapig lay down, but stirred when the jar was moved. It was allowed to remain in the jar for half an hour, being asleep except when disturbed. When taken out it awoke and endeavoured to walk, but was unable to support itself at first. It flinched on being pricked. Recovered in three or four minutes.
Experiment 4. A cat was placed in the same jar, and the same quantity of chloroform was introduced. In three minutes it had evaporated, and, when ten minutes had elapsed, the cat began to stagger. Soon afterwards it was unable to support itself on its legs; and, when a quarter of an hour had elapsed, it seemed asleep, but raised its head when the jar was inclined. It remained apparently sleeping till the end of an hour, when it was taken out. It was unable to stand, but was sensible to the slightest pinch. It recovered gradually in the course of twenty minutes.
Experiment 5. Sixteen grains of chloroform were put into a jar holding 1,600 cubic inches, being one grain to each 100 cubic inches of air, as in the two last experiments. When it was converted into vapour, a white mouse was introduced, by moving the lid a little to one side for a moment. After running about for a minute and a half, it began to stagger and to lose power, but it continued to run with little intermission till three minutes had expired. After this it lay still, except when the jar was inclined, when it always endeavoured to maintain its balance and to walk. It [61/62] also moved its limbs now and then, when not disturbed. It was removed at the end of ten minutes, when it tried to walk, but was unable. It did not flinch when its tail was pinched, but flinched, half a minute after its removal, on one of its toes being pinched. It recovered in two or three minutes.
Experiment 6. A guineapig was placed in the jar holding 3,000 cubic inches, and 37.5 grains of chloroform were introduced in the same manner as in the former experiments, being a grain and a quarter to each 100 cubic inches of air. The chloroform took three or four minutes to evaporate and diffuse itself in the jar; and by the end of this time the guineapig, which had been excited and running about, began to stagger, and in two minutes longer it was unable to walk, but endeavoured to keep its balance when the jar was inclined. At the end of a quarter of an hour it was lying still, but moved its limbs when it was rolled over by inclining the jar; but it made no voluntary effort. It was taken out when thirty-three minutes had elapsed. It moved its limbs as it was removed, though apparently not in a voluntary manner. Its limbs were not relaxed. It was quite insensible to pricking. It recovered in about ten minutes. The temperature in the axilla before it was put into the jar was 100° Fah., and immediately after its removal 96°.
Experiment 7. A guineapig was placed in the same jar, and forty-five grains of chloroform were introduced, being a grain and a half to each 100 cubic inches of air. In four minutes after the chloroform had evaporated, the guineapig was unable to walk. In half a minute more it seemed asleep, but there was a tremulous motion of the hind legs, which continued till ten minutes had elapsed. Afterwards it lay still, but winked now and then spontaneously. When rolled over by moving the jar, it made no voluntary effort. It was taken out twenty minutes after the chloroform had evapo-[62/63] rated. It winked spontaneously, and also when the eyes were touched. It did not flinch when the ear was pricked, but flinched when the paw was pricked. The temperature in the axilla before the experiment was 100°, and immediately afterwards it was 96°. The guineapig recovered from the effects of the chloroform in ten minutes.
Experiment 8. A guineapig was put into the same jar, and 52.5 grains of chloroform were introduced, being a grain and three quarters to each 100 cubic inches of air. The chloroform evaporated in the course of four minutes, at the end of which time the guineapig was altered in its manner, as if partially inebriated. In two minutes more it was becoming drowsy. A little while afterwards it was lying down. Six minutes after the evaporation of the chloroform was complete, the guineapig made no effort when turned over by inclining the jar, but only moved its feet, as it were automatically. At the end of nine minutes, it was lying quietly and breathing naturally. When fifteen minutes had elapsed it was in the same condition, and was removed from the jar. It cried and flinched on the foot being pricked. The temperature in the axilla was 97°. In five minutes after its removal it was fast recovering, and in ten minutes was quite recovered.
Experiment 9. A guineapig was placed in the jar used in the last three experiments, and sixty grains of chloroform were introduced in the same manner, being two grains to each 100 cubic inches of air. In four minutes it was all converted into vapour, and the guineapig was beginning to be affected by it. In two minutes more it was unable to stand or walk. In five minutes from the time when the evaporation was complete, the guineapig showed no sign of sensibility when turned over by inclining the jar; the breathing was natural. At the end of ten minutes it was lying still, breathing gently forty times in the minute. At [63/64] the end of fifteen minutes it was in the same condition. From seventeen to twenty minutes, it stretched out one of its hind legs several times, and was doing so when taken out, at the end of twenty minutes. It showed no sign of sensibility when pricked. The temperature in the axilla was 96°. It began to recover gradually in a minute or two, and recovered completely in from ten to fifteen minutes.
Experiment 10. A cat was placed in the same jar, and the same quantity of chloroform was introduced in the same manner. It became quite insensible in a few minutes after the chloroform was introduced; and it was allowed to remain for twenty-five minutes, when it was taken out. It was perfectly insensible to pricking, and its muscles were quite relaxed; it was breathing gently, and the pulsations of the heart were between sixty and seventy in the minute. It was immediately made the subject of another experiment of drowning whilst insensible, which need not be related in this place.
Experiment 11. Four grains of chloroform were put into a glass jar holding 200 cubic inches, and when it had evaporated and was diffused through the air in the jar, a white mouse was introduced, by momentarily removing the cover a little to one side. A minute after its introduction the mouse was lying, but it moved its legs for a quarter of a minute longer. When four minutes had elapsed, the breathing became slow, and it was taken out. It was totally insensible for the first three minutes after its removal, and recovered during the two following minutes.
Experiment 12. Thirty-two grains of chloroform were diffused through the air of a jar holding 1,600 cubic inches, being two grains to each 100 cubic inches, as in the last three experiments. A white mouse was introduced by moving the cover a little to one side for a moment. In one minute it was insensible, and did not make any effort on [64/65] being rolled about by inclining the jar, but it moved its paws for half a minute longer. It remained insensible, breathing 160 times in the minute, till it was taken out at the end of five minutes. It was quite insensible to pinching. It began to walk in a minute or two. Its temperature before the experiment was 98°, and immediately afterwards was 92°. The temperature of the room was 68°.
Experiment 13. A guineapig was put into a jar holding 3,000 cubic inches, and 67.5 grains of chloroform were introduced on blotting paper suspended within the jar, being 21 grains to each 100 cubic inches. In four minutes, the chloroform had all evaporated, and the guineapig was becoming affected. In two minutes more, it was quite insensible. Eight minutes after the chloroform had evaporated, it was lying still, breathing forty times in the minute. During the next three or four minutes, it moved one or other of its legs occasionally. At the end of seventeen minutes, it was lying still, and the breathing was twenty-six in the minute. It was taken out at the end of twenty minutes quite insensible; in three or four minutes it began to try to walk, and in ten minutes, was quite recovered.
Experiment 14. Two white mice, one being full grown, and the other about three-quarters grown, were placed in the jar holding 1,600 cubic inches, and forty grains of chloroform were introduced on blotting paper, being two grains and a half to each hundred cubic inches. In two minutes, the chloroform had evaporated, and the mice were much excited. In another minute, they were unsteady in walking; and in a minute more, the old mouse was lying insensible, and breathing deeply and laboriously. In four minutes more, i.e., six minutes after the chloroform had evaporated, the young mouse was insensible also, but was moving one of its hind legs. In other four minutes, the young mouse was breathing by slow gasps, whilst the old one continued [65/66] to breathe deeply as before. Three minutes later, i.e., thirteen minutes after the chloroform had evaporated, the old mouse had begun to gasp, and the young one was gasping only at intervals. They were removed, and recovered completely in ten minutes. The young one recovered most quickly. Their temperature, on being removed, was about 90°.
Experiment 15. A cat was put into the jar holding 3,000 cubic inches, and 82.5 grains of chloroform were introduced, being two grains and three-quarters to each hundred cubic inches. In five minutes, it had evaporated, and the cat began to stagger in its walk. In two minutes more, it was unable to stand. Five minutes after the chloroform had evaporated, the cat was breathing deeply, seventy-five times in the minute. At eight minutes, it was breathing less deeply, one hundred and seventeen times in the minute. Ten minutes after the chloroform had evaporated, the cat was quite insensible, and breathing one hundred and twenty-six times in the minute. It was now taken out. The temperature in the axilla was 98°. In half an hour after its removal from the jar, it had recovered its consciousness, but was still drowsy.
It was now put into the jar again, and the same quantity of chloroform was introduced in the same manner as before. In five minutes, it had evaporated, and the cat was again insensible. In other five minutes, it was breathing rather deeply, forty-eight times in the minute. Twelve minutes after the chloroform had evaporated, the cat was breathing in the same manner, but sixty-eight times in the minute. The breathing afterwards became shallow and feeble, and half an hour after the chloroform had evaporated, it was eighty-eight in the minute. In five minutes more, the breathing ceased. The cat was taken out of the jar, and the stethoscope was applied to the chest. The heart could not be heard to beat at first, but in a short time, the cat [66/67] gave a gasp, and the heart's action returned, and the breathing became re-established.
Experiment 16. Forty-eight grains of chloroform were put into a jar holding 1,600 cubic inches, being three grains to each hundred cubic inches, and when it was converted into vapour and diffused through the air in the jar, a white mouse was introduced. It ran about for a minute and a half, and then it was unable to move any longer. In nine minutes and a half, the breathing was getting very slow, and the mouse was immediately removed. Before it could be got out, it appeared to have entirely ceased to breathe, but it immediately began to gasp at intervals. In a minute, the breathing improved, and soon became natural. Three minutes after its removal, the mouse began to walk in a ring, and in seven minutes, it had quite recovered.
Experiment 17. A guineapig was placed in a jar holding 1,600 cubic inches, and fifty-four grains of chloroform were introduced on blotting paper, in the manner previously explained; being three grains and three-eighths to each hundred cubic inches of air. In four minutes, the chloroform had evaporated, and become diffused through the air in the jar, and the guineapig was drowsy. In three minutes more, it was lying apparently insensible, and breathing feebly, thirty times in the minute. After this, it kicked occasionally for a few minutes. When six minutes had elapsed from the time when the chloroform had evaporated, the breathing was very feeble, and apparently performed only by the diaphragm. From fifteen to eighteen minutes, I could hardly see whether the animal was breathing or not, and it was taken out of the glass at eighteen minutes, when the breathing appeared to have ceased. The stethoscope was applied to the chest, and the sounds of the heart could scarcely be heard at first, but the breathing returned in a few seconds, and the action of the heart im-[67/68]proved. The guineapig gradually recovered, but it was not able to walk for twenty-five minutes.
Experiment 18. Sixty grains of chloroform were introduced into the jar employed in the last experiment, being three grains and three-quarters to each hundred cubic inches of air contained in the jar. When it had evaporated, and was diffused through the air, a white mouse was introduced, whilst the lid of the jar was moved a little to one side for a moment. It ran about at first, but suddenly ceased to run, and became insensible, at the end of three-quarters of a minute. It lay breathing deeply and rapidly till two minutes had elapsed, when the respiration became slow, and it ceased at two minutes and three-quarters after the mouse was introduced. It was removed at this time, and it gasped a few seconds afterwards; this gasp was soon followed by another; the gaspings became more frequent, and in a short time, the natural breathing was resumed. In five minutes, the mouse was able to walk.
The third, fourth, and fifth of the above experiments show that one grain of chloroform to each hundred cubic inches of air suffices to induce the second degree of narcotism, or that state in which consciousness and voluntary motion are disturbed, but not entirely abolished. Now one grain of chloroform produces 0.767 of a cubic inch of vapour at 60°, when its specific gravity is 4.2; and, when the vapour is inhaled, it expands somewhat, as it is warmed to the temperature of the lungs; but it expands only to the same extent as the air with which it is mixed, and therefore the proportions remain unaltered. But air, when saturated with vapour of chloroform at 100°, contains 43.3 cubic inches in 100; and
So that if the point of complete saturation be considered as unity, 0.0177 or 1-56th, will express the degree of satu-[68/69]ration of the air from which the vapour is immediately absorbed into the blood; and, consequently, also the degree of saturation of the blood itself.
I find that serum of blood at 100?, and at the ordinary pressure of the atmosphere, will dissolve about its own volume of vapour of chloroform; and since chloroform of specific gravity 1.483 is 288 times as heavy as its own vapour, 0.0177 ÷ 288 gives 0.0000614, or one part in 16,285, as the average proportion of chloroform by measure in the blood, in the second degree of narcotism.
It is evident, from the experiments numbered 9 to 12 inclusive, that two grains of chloroform to each hundred cubic inches of the inspired air cause a state of very complete insensibility, corresponding with what I have designated the fourth degree of narcotism; and by the method of calculation employed above we get 0.0354, or 1-28th, as representing the degree of saturation of the blood, and 0.0001228 the proportion by measure in the blood.
In experiments 6, 7, and 8, in which quantities of chloroform were employed intermediate between one and two grains to each hundred cubic inches of air, a moderate amount of insensibility was induced, corresponding very much with the state of patients during operations under chloroform.
The experiments from 13 to 18 show that quantities of chloroform, exceeding two grains to 100 cubic inches of air, have a tendency to embarrass and arrest the function of respiration, if the inhalation is continued. I have not yet been able to determine satisfactorily the exact proportion of chloroform which requires to be absorbed to arrest the respiration of animals of warm blood. I believe there is a definite proportion which has this effect, but there are two reasons why it is not so easy to ascertain it, as to ascertain the proportion which causes the minor degrees of narcotism. [69/70] In the first place, the breathing often becomes very feeble before it ceases, so that the animal inhales and absorbs but very little chloroform, and remains on the brink of dying for some time. In the next place, the temperature of the body falls in a deep state of narcotism, especially in small animals; and, as the temperature falls, the amount of chloroform which the blood can dissolve from any given mixture of air and vapour increases.
Judging from the experiments numbered 14 to 18, three grains of chloroform to each hundred cubic inches of air must be very nearly the quantity which has the power of arresting the breathing when the temperature of the body is 100°; and as three grains of chloroform produce 2.3 cubic inches of vapour, and air at 100° is capable of taking up 43.3 per cent of its volume, it follows that the blood must contain between 1-18th and 1-19th as much chloroform as it is capable of dissolving, at the time when the respiration is arrested. In the 14th experiment, the breathing of the two mice was on the point of being stopped by two and a half grains of chloroform in each hundred cubic inches of air, but during the thirteen minutes which the mice breathed the vapour, their temperature fell to about 90°. Air, when saturated with the vapour of chloroform at this temperature, contains 35 per cent, and two grains and a half of chloroform yield 1.917 cubic inches of vapour; so by a calculation similar to that made at page 68, the mice at the time when the breathing was about to cease must have absorbed 1-18th part as much chloroform as their circulating fluids were capable of dissolving.
The reader will have observed that, in the experiments related above, the mice became much more quickly affected than the guineapigs and cats. The reason of this is their quicker respiration and circulation, and much more diminutive size. Little birds, such as linnets and sparrows, are [70/71] also very quickly affected by chloroform. Frogs are more slowly affected, owing to their languid respiration, unless the vapour to which they are exposed is very strong.
They can, however, owing to their low temperature, be rendered insensible by proportions of vapour too small to affect animals of warm blood; and as they have no proper temperature of their own, the amount of vapour (in proportion to the air in which they are placed) that will affect them, depends entirely on the temperature of that air.
The following experiment was several times performed on frogs with the same result, the temperature of the room being about 55°, as it was in winter.
Experiment 19. 4.6 grains of chloroform were diffused through the air of a jar of the capacity of 920 cubic inches, and a frog was introduced. In a few minutes, it became affected, and at the end of ten minutes, was quite motionless and flaccid; but the respiration was still going on. Being now taken out, it was found to be insensible to pricking: it recovered in a quarter of an hour.
In a repetition of this experiment, in which the frog continued a few minutes longer in the vapour, the respiration ceased, and the recovery was more tardy. On one occasion, the frog was left in the jar for an hour, but when taken out, and turned on its back, the pulsations of the heart could be seen. In an hour after its removal, it was found to be completely recovered.
The first of the experiments related above (page 60), showed that an atmosphere containing half a grain of chloroform to each hundred cubic inches, produced scarcely any appreciable effect on animals of warm blood; but the following calculation explains why this quantity acts so energetically on the frog, and proves that this creature is affected by chloroform according to the same law as animals of warm blood. The vapour is absorbed into the blood and [71/72] lymph of the frog at the temperature of the external air, whose point of relative saturation therefore remains unaltered, both in the lungs and in contact with the skin of the animal; and as half a grain of chloroform produces 0.383 cubic inches of vapour, and air at 55° contains, when saturated, 10 per cent of vapour; 0.0383, or 1-26th, expresses the degree of saturation of the air, and also of the blood of the frog. And this is a very little more than the quantity (0.0354 or 1-28th) which was calculated above to be the greatest amount which could be absorbed with safety into the blood of the mammalia. It must be observed, however, that the pulmonary respiration of the frog was arrested by this proportion of 1-26th as much chloroform as the blood would dissolve, whilst we calculated that it required about as much as 1-18th to arrest the breathing of animals of warm blood. It must be remembered, however, that the pulmonary respiration of frogs is a process of swallowing air, which only goes on when the creature is comparatively active. In the torpid state, the respiration takes place only by the skin, and the frog never breathes with the aid of the same muscles and nerves as mammalia and birds.
By warming a frog, together with the air in which it is placed, it is, in accordance with the law explained above, rendered comparatively proof against an amount of chloroform which would otherwise render it insensible.
Experiment 20. A frog, which had been a few days previously subjected to the experiment just narrated, was put into the same jar, which was placed near the fire, till a thermometer inside marked 75° Fah.; 4.6 grains of chloroform were then introduced, and diffused through the air in the jar. The jar was kept for twenty minutes, with the thermometer indicating the same temperature within one degree. For the first seventeen minutes, the frog was unaffected; and only was dull and sluggish, but not insensible, [72/73] when taken out. Air at 75°, when saturated with vapour of chloroform, contains 22 per cent, and therefore the 0.383 per cent of vapour, which at 55° was capable of saturating the fluids of the frog to the extent of 1-26th of what they would dissolve, was, at 75°, capable of saturating them only to the extent of 1-57th.
At one of Dr. Wilson's Lumleian Lectures, at the College of Physicians, on March 29th, 1848, I had the honour of performing some experiments, and making some remarks, on chloroform, and I combined together two experiments on frogs and small birds, in a way which shows how entirely the effects of a narcotic vapour depend on the quantity of air with which it is mixed, and on other physical conditions.
Experiment 21. I introduced a chaffinch, in a very small cage, into a glass jar holding nearly 1,000 cubic inches, and put a frog into the same jar, covered it with a plate of glass, and dropped five grains of chloroform on a piece of blotting paper suspended within. In less than ten minutes, the frog was insensible, but the bird was not affected.
Experiment 22. I then placed another frog and another small bird in a jar containing but 200 cubic inches, with exactly the same quantity of chloroform. In about a minute and a half, they were both taken out,--the bird totally insensible, but the frog not appreciably affected, as from its less active respiration it had not had time to absorb much of the vapour.
The blood in the human adult is estimated by M. Valentin to average about thirty pounds. M. Valentin's experiments were so conducted that this quantity must include the extra vascular liquor sanguinis, as well as the blood actually contained within the vessels. On this account, his estimate is all the better fitted for calculating the amount of chloroform absorbed, since this medicine, when inhaled gradually, passes by exosmosis through the coats of the blood-[73/74] vessels into the fluid in which the tissues are immediately bathed. The above quantity of blood would contain 26 pounds 5 ounces of serum, which, allowing for its specific gravity, would measure 410 fluid ounces. This being reduced to minims, and multiplied by 0.0000614, the proportion of chloroform in the blood required to produce narcotism to the second degree (see page 68), gives 12 minims as the whole quantity in the blood. More than this is used in practice, because a considerable portion is not absorbed, being thrown out again when it has proceeded no further than the trachea, the mouth and nostrils, or even the face-piece. But I find that if I put twelve minims into a bladder containing a little air, and breathe it over and over again, in the manner of taking nitrous oxide, it suffices to remove consciousness, producing the second degree of its effects.
To induce the third degree of narcotism, or the condition in which surgical operations are usually commenced, would require that about 18 minims should be absorbed by an adult of average size and health, according to the above method of calculation; and to induce the deep state of insensibility, which I have termed the fourth degree of narcotism, would require 24 minims; whilst to arrest the function of respiration would require that about 36 minims should be absorbed.
The only direction which it is usually requisite to give beforehand, to the patient who is to inhale chloroform, is to avoid taking a meal previous to the inhalation; for chloroform is very apt to cause vomiting, if inhaled whilst there is a quantity of food in the stomach. The sickness is not attended with any danger, but it constitutes an unpleasantness and inconvenience which it is desirable to avoid. The best time of all for an operation under chloroform is before [74/75] breakfast, but the customs and arrangements of this country do not often admit of that time being chosen, and it is unadvisable to make the patient fast beyond his usual hour. It answers very well to perform an operation about the time when the patient would be ready for another meal, or, if the time of operation fall two or three hours after the usual time of eating, to request the patient to make only a slender repast at that time, so as just to prevent the feeling of hunger. It is impossible to prevent vomiting in some cases with the best precautions, for the stomach occasionally will not digest when the patient is expecting a surgical operation, and the breakfast may be rejected in an unaltered state hours after it has been taken. In other cases the patient does not vomit, even when he inhales chloroform shortly after a full meal.
The most convenient position in which the patient can be placed whilst taking chloroform is lying on the back, or side, as he is then duly supported in the state of insensibility, and can be more easily restrained if he struggle whilst becoming insensible. The semi-recumbent posture on a sofa does very well, and there is no objection to the sitting posture, when that is most convenient to the operator. In that case, however, the patient should be placed in a large easy chair with a high back, so that the head as well as the trunk may be supported without any effort, otherwise he would have a tendency to slide or fall when insensible. It has been said that it is unsafe to give chloroform in the sitting posture, on the supposition that it would in some cases so weaken the power of the heart, as to render it unable to send the blood to the brain. Observation has proved, however, that chloroform usually increases the force of the circulation; and although the horizontal position is certainly the best for the patient under an operation in all circumstances, I consider that the sitting posture is by no [75/76] means a source of danger, when chloroform is given, if the ordinary precaution be used, which would be used without chloroform--that of placing the patient horizontally if symptoms of faintness come on. I have preserved notes of nine hundred and forty-nine cases in which I have given chloroform to patients in the sitting posture, and no ill effects have arisen in any of these cases.
The person who is about to inhale chloroform is occasionally in a state of alarm, either about that agent itself or the operation which calls for its use. It is desirable to allay the patient's fears, if possible, before he begins to inhale, as he will then be able to breathe in a more regular and tranquil manner. In a few cases, however, the apprehensions of the patient cannot be removed, and they subside only as he becomes unconscious from the inhalation. It has been said that chloroform ought not to be administered if the patient is very much afraid, on the supposition that fear makes the chloroform dangerous. This is, however, a mistake; the danger, if any, lies in the fear itself. Two cases will be related hereafter in which the patients died suddenly from fear, whilst they were beginning to inhale chloroform, and before they were affected by it; but the probability is that, if they had lived till the chloroform took effect, they would have been as safe as other patients who inhaled it. If chloroform were denied to the patients who are much afraid, the nervous and feeble, who most require it, would often be deprived of its benefits. Moreover, the patients would either be prevented altogether from having the advantage of surgery, or they would be subjected to the still greater fear of the pain, as well as the pain itself; for whatever undefined and unreasoning fears a patient may have when the moment comes for inhaling chloroform, he has only chosen to inhale it on account of a still greater fear of pain. [76/77]
Fear and chloroform are each of them capable of causing death, just as infancy and old age both predispose to bronchitis, but it seems impossible that fear should combine with the effects of chloroform to cause danger, when that agent is administered with the usual precautions. Fear is an affection of the mind, and can no longer exist when the patient is unconscious; but the action of that amount of chloroform which is consistent even with disordered consciousness is stimulating, and increases the force and frequency of the pulse, in the same way as alcohol. I believe that no one would assert that a person would die the sooner of fright for having taken a few glasses of wine, or a small amount of distilled spirits, whatever might be the state of his health. When chloroform has been absorbed in sufficient quantity to cause unconsciousness, fear subsides, and with the fear its effects on the circulation. It is a subject of almost daily observation with me that the pulse, which is extremely rapid from some ill defined apprehension, when certain patients begin to inhale chloroform, settles down to its natural frequency after they become unconscious.
The practice I have always followed has been to try to calm the patient, by the assurance that there was nothing to apprehend from the chloroform, and that it would be sure to prevent all pain; but where it has been impossible to remove the fears of the patient in this way, I have always proceeded to remove them by causing a state of unconsciousness. It would of course be wrong to choose a moment for beginning the inhalation, when fear was producing a very marked depression of the circulation. On feeling the pulse of a gentleman, about twenty-one years of age, in March 1855, who had just seated himself in the chair to take chloroform, previous to having some teeth extracted, by Mr. Thos. A. Rogers, I found it to be small, weak, and intermitting, and it became more feeble as I was feeling it. [77/78]
I told the patient that he would feel no pain, and that he had nothing whatever to apprehend. His pulse immediately improved. He inhaled the chloroform, had his teeth extracted, woke up, and recovered without any feeling of depression. Now if the inhalation had been commenced in this case, without inquiry or explanation, the syncope which seemed approaching would probably have taken place, and it would have had the appearance of being caused by the chloroform, although not so in reality.
The experiments previously related show that air containing rather less than two grains of chloroform, in one hundred cubic inches, is capable of causing a state of insensibility, sufficiently deep for surgical operations but in a creature the size of the human being, an inconvenient length of time would be occupied in causing insensibility with vapour so much diluted. About four cubic inches of vapour, or rather more than five grains of chloroform to each hundred cubic inches of air, is the proportion which I have found most suitable in practice for causing insensibility to surgical operations. In medical and obstetric cases, it should be inhaled in a more diluted form.
Dr. Simpson recommended chloroform to be administered on a handkerchief--the method in which sulphuric ether was administered by Dr. Morton, in the first case in which he exhibited that medicine. The objection to giving chloroform on a handkerchief, especially in surgical operations, where it is necessary to cause insensibility, is that the proportions of vapour and of air which the patient breathes cannot be properly regulated. Indeed, the advocates of this plan proceed on the supposition that there is no occasion to regulate these proportions, and that it is only requisite that the patient should have sufficient air for the purposes of [78/79] respiration, and sufficient chloroform to induce insensibility, and all will be right.43 The truth is, however, that if there be too much vapour of chloroform in the air the patient breathes, it may cause sudden death, even without previous insensibility, and whilst the blood in the lungs is of a florid colour. Chloroform may indeed be inhaled freely from a handkerchief without danger, when it is diluted with one or two parts by measure of spirits of wine, but the chloroform evaporates in largest quantity at first, and less afterwards, until a portion of the spirit is left behind by itself. The process, however, of inhaling chloroform from a handkerchief is always uncertain and irregular, and is apt to confirm the belief in peculiarities of constitution, idiosyncrasies and predispositions, which have no existence in the patient. 43a [79/80]
The most exact way in which it is practicable to exhibit chloroform to a patient about to undergo an operation, is to introduce a measured quantity into a bag or balloon of known size, then to fill it up by means of the bellows, and allow the patient to inhale from it; the expired air being prevented from returning into the balloon, by one of the valves of the face-piece to which it is attached. I tried this plan in a few cases, in 1849, with so much chloroform in the balloon as produced four per cent of vapour in proportion to the air. The effects were extremely uniform, the patients becoming insensible in three or four minutes, according to the greater or less freedom of respiration; and the vapour was easily breathed, owing to its being so equally mixed with the air. I did not try, however, to introduce this plan into general use, as the balloon would sometimes have been in the way of the surgeon, and filling it with the bellows would have occasioned a little trouble. It seemed necessary to sacrifice a little of absolute perfection to convenience, and I therefore continued the plan which I had already followed.
The great point to be observed in causing insensibility by any narcotic vapour, is to present to the patient such a mixture of vapour and air as will produce its effects gradually, and enable the medical man to stop at the right moment. Insensibility is not caused so much by giving a dose as by performing a process. Nature supplies but one mixture of diluted oxygen, from which each creature draws as much as it requires, and so, in causing narcotism by inhalation, if a proper mixture of air and vapour is supplied, each patient will gradually inhale the requisite quantity of the latter to cause insensibility, according to his size and strength. It is indeed desirable to vary the proportions of vapour and air, but rather according to the purpose one has in view, whether medicinal, obstetric, or surgical, than on [80/81] account of the age or strength of the patient; for the respiratory process bears such a relation to the latter circumstances, as to cause each person to draw his own proper dose from a similar atmosphere in a suitable time.
The inhaler represented in the adjoining engraving is, with some slight alterations, the same that I have employed since the latter part of 1847. It is made of metal, and consists of a double cylinder, the outer space of which contains cold water, and the inner serves for the evaporation of the chloroform which the patient is to breathe. Into the inner part of the cylinder there is screwed a frame, having numerous openings for the admission of air, and four stout wires which descend nearly to the bottom of the space, and are intended to support two coils of stout bibulous paper, which are tied round them, and reach to the bottom of the inhaler. In the lower part of this paper four notches are cut, to allow the air to pass in the direction indicated by the arrows. As the quantity of chloroform which is put in should never fill the apertures or notches, the air which passes through the inhaler meets with no obstruction whatever. There is a glass tube communicating with the interior of the inhaler, and passing to the outside, to enable the operator to see when the chloroform requires to be renewed. The elastic tube which connects the inhaler to the face-piece is three-quarters of an inch in internal diameter, to allow of the passage of as much air as the patient can possibly breathe. On the introduction of the practice of inhaling sulphuric ether there was no tubing in this country fit to be breathed through; that in ordinary use was only about one-third, or three-eighths of an inch in diameter,--not more than a quarter of the proper calibre.
The face-piece, to include both the mouth and nostrils, of which that shown in the engraving is one of the modifications, is one of the greatest mechanical aids to the process [81/82]
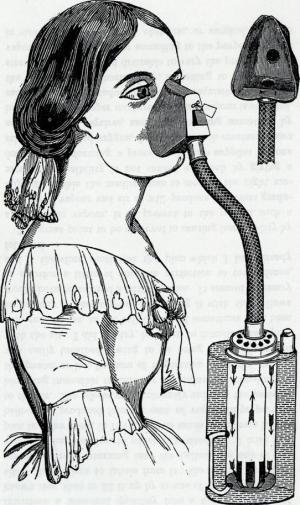
[82/83] of inhalation which has been contrived in modern times. Dr. Francis Sibson is its inventor. Dr. Hawkesley did indeed contrive a very similar one about the same time as Dr. Sibson,--early in 1847,--but he did not make it known. Dr. Ingen Housz made patients inhale oxygen through the nostrils by means of a bottle of India rubber with the bottom cut off; and Mr. Waugh, of Regent Street, had more recently contrived a mouth-piece to be adapted outside the lips, but the usual practice of inhalation previous to 1847, was for the patient to draw in the medicated air by means of a tube placed in the mouth. This led generally to great awkwardness at first, as the patient usually began to puff as if he were smoking a pipe; and it had the further inconvenience, in the administration of ether, that the tube dropped from the mouth, and the patient began to breathe by the nostrils, just as he was getting unconscious. The sides of the face-piece delineated in the engraving are made of thin sheet lead, which is pliable, and enables it to be adapted exactly to the inequalities of the face, and the patient can breathe either by the nostrils or mouth, just as his will, or instinct, or other nervous functions, determine.
I have introduced two valves into this face-piece, one which rises on inspiration, to admit the air and vapour from the inhaler, and closes again on expiration, and the other which rises to allow the expired air to escape. I contrived the latter valve to turn more or less to one side, as indicated by the additional line in the engraving, and thus admit more or less of the external air to dilute still further that which has passed through the inhaler, and become charged with vapour. By this means the patient can begin by breathing air containing very little vapour, and more and more of the air which has passed over the moistened bibulous paper can be admitted, as the air passages become blunted to the pungency of the vapour. [83/84]
The object of the water bath is to supply the caloric which is rendered latent, and carried off, as the chloroform is converted into vapour, and thus to render the process of inhalation steady and uniform. Without the water bath, the evaporation of the chloroform would soon reduce the temperature of the inhaler below the freezing point of water, and limit very much the amount of vapour the patient would inhale; and if the apparatus were warmed by the hand, the temperature would be too high, and the amount of vapour too great. A medical author of great reputation in Paris sent to inquire at what temperature I used the water bath, and being informed, at the ordinary temperature, published his opinion that it had no effect, and might as well be left off. He appeared not to have considered the relations of heat, either to liquids or vapours.
In arranging the bibulous paper in the inhaler, it is my object to contrive that the air passing through, in the ordinary process of inhalation, and at the ordinary temperature of about 60?, shall take up about five per cent of vapour. This quantity can be diminished, as much as is desired, by turning the expiratory valve of the face-piece a little to one side; and in winter I usually place a short coil of bibulous paper against the outer circumference of the inside of the inhaler, in addition to the central coils which are delineated.
I commonly put two, or two and a half, fluid drachms of chloroform into the inhaler at first. About a drachm of this is absorbed by the filtering paper, and the rest remains at the bottom of the inhaler; and in a protracted operation, when it is seen, by means of the glass tube, that the latter part of the chloroform has disappeared, more is added, by a drachm or so at a time, to prevent the paper ever becoming dry. Mr. Matthews, 8, Portugal Street, Lincoln's Inn Fields, makes the inhaler. There are smaller face-pieces for [84/85] children. The patient never inhales in so upright a posture as the artist has represented.
There are several other kinds of apparatus in use for the inhalation of chloroform. The most usual consist of Dr. Sibson's face-piece more or less altered, and with a small piece of sponge placed inside. The apparatus which is in most reputation on the continent is that of M. Charrière; it consists of a glass vase with suitable valves, and a fabric for exposing a surface wetted with chloroform to the air which passes through it.
M. Duroy, of Paris, has contrived an ingenious, but very complicated, apparatus, which he calls an anæsthesimeter. The object of it is to regulate the amount of chloroform which is inhaled in a given time, and this can be varied from four to sixty drops in the minute; but the experiments which I have related show that the quantity of chloroform employed is not so important as the proportion of it in the inspired air; and although each of these circumstances has considerable influence over the other, in many cases there are conditions in which no regular relation exists between them. For instance, if the inhaler were supplied with sixty drops of chloroform per minute, these sixty drops weigh twenty grains, and produce 15.3 cubic inches of vapour; and if an adult patient were breathing the average quantity of four hundred cubic inches per minute, the air he would breathe would contain nearly four per cent of vapour, which would answer extremely well; but if the breathing were slow or feeble, or if he should hold his breath for an interval and commence again, he might breathe air much more highly charged with vapour. Indeed it would depend on the amount of surface moistened with chloroform, the temperature of the air, and other physical conditions, whether or not the air he inhaled might not be charged with chloroform to a dangerous degree; whilst, on the other hand, if [85/86] the breathing were deep and rapid, as often happens whilst the patient is getting slightly under the influence of the chloroform;--if, for instance, the patient were to breathe at the rate of 1,600 cubic inches, instead of 400, the air he would inhale would contain less than one per cent of vapour, and he would not become insensible with the utmost supply of the anæsthesimeter, till his breathing should be moderated. M. Duroy also follows the rude and objectionable plan of using a nose clasp, and thus compelling the patient to breathe by the mouth alone.
It is advisable to request the patient to breathe gently and quietly, when he commences to inhale chloroform; in other words, to do nothing but conduct himself as if he were about to fall asleep naturally; for, if he breathes deeply, the vapour feels much more pungent than it otherwise would do, and is apt to excite coughing, or a feeling of suffocation.
In using the inhaler described above, the patient should commence to inhale with the expiratory valve of the face-piece turned on one side, and it should be gradually advanced to the required extent, over the opening it is intended to cover, as the sensibility of the lungs becomes diminished. Not only patients with phthisis or bronchitis, but many sensitive and irritable persons with sound lungs, have a great intolerance of the vapour of chloroform at first, on account of its pungency; and it is necessary to occupy two or three minutes in gradually commencing the inhalation, before the patient makes any appreciable progress towards insensibility. In administering chloroform to children also, it is desirable to begin very gently; by this means, and with a little persuasion, one generally succeeds in getting them to inhale voluntarily; although, occasionally, it is necessary to use a little force to accomplish one's purpose. [86/87]
In certain cases of the medicinal application of chloroform, and also in obstetric cases, where the pains are not severe, it is unnecessary to render the patient unconscious, but for surgical operations this is nearly always requisite. No force should ever be employed so long as the patient is conscious, unless it be to children or lunatics; but some patients become excited as soon as they are unconscious, and attempt to leave the couch, or push away the chloroform under such circumstances, if they cannot be calmed by what is said to them, they should be held, and the vapour should be steadily and gently continued, for a minute or two, till a state of quietude is produced. By far the greater number of patients remain quiet as they become unconscious, but there is no difficulty in ascertaining whether a patient is unconscious or not. If the eyelids remain open, the countenance shows whether the patient is conscious or not and, if they are closed, it is only necessary to touch them gently, to ascertain this circumstance. If he is still conscious, he will look at his medical man, and probably speak, or, at all events, show intelligence in his countenance.
Signs of Insensibility. The absence of consciousness, and a state of quietude, are both requisite before the commencement of a surgical operation, and they go a good way towards the preparation of a patient for it, but these symptoms may be present and the patient not be ready for an operation. The surgeon wishes to know whether he will lie still under the knife, or whether he will make a resistance and outcry which he would probably not make in his waking state. Some surgeons have recommended that the patient should be pricked with the point of a knife or some other instrument. This is not a good or satisfactory plan, however, for a person will often show no sign of feeling a slight prick, when a severe incision would rouse him to resistance. A more elegant and successful plan [87/88] is to raise the eyelid gently, by placing one finger just below the eyebrow, and then to touch its ciliary border very lightly with another finger. This should not be done roughly nor too frequently, for fear of exhausting the sensibility when it is slight. Just after unconsciousness is induced, the eyelids are often closed very strongly when their margins are touched, especially in females, and there seems to be a positive hyperæsthesia; this, however, is only apparent, and arises from the control of the will being removed, whilst sensibility remains. By continuing the chloroform, the sensibility of the edges of the eyelids diminishes until, at last, they may be touched without causing winking. Under these circumstances, the most severe operation may, in almost every case, be commenced without sign of pain. I have employed this test of the sensibility or insensibility of the patient ever since chloroform has been in use, and also in the employment of ether in 1847, and I am satisfied that it affords more reliable information on this point than any other single symptom. It even indicates the amount of sensibility where a little remains; when, for instance, touching the margin of the eyelids causes very slight and languid winking, the patient will commonly flinch a little if the knife is used, but only in a manner that can be easily restrained, and will not interfere with the majority of operations. The cases, in which the indication afforded by the eyelids is not always to be depended on, are those of hysterical patients, in whom there is sometimes no winking on touching the eyelids, even when unconsciousness is scarcely induced. In such cases, one must judge by the other symptoms, and also by the length of time the patient has inhaled, the strength of the vapour, and depth and activity of the breathing. Indeed, these conditions should be observed and taken into account in every case; and all the symptoms exhibited by the patient should be watched, such [88/89] as the expression of the face, the state of the breathing, and the condition of the limbs with regard to their tension or relaxation. The last is indeed sometimes relied on as the chief or sole sign whether the operation may be commenced, but it is of itself very insufficient, and even fallacious. The patient may allow his limbs to lie relaxed when he is scarcely unconscious, and not at all insensible, merely because he is not exerting his will upon them if the arm is lifted, it may fall listlessly down again, at a time when the knife of the surgeon would rouse the patient to active resistance. Indeed, the limbs, which have been lying relaxed, may become tense as the effect of the chloroform increases, and may remain so during a short operation, in which there is no sign of pain.
Although the pulse of itself gives no indication as to how far a patient is under the influence of chloroform, it is proper to pay attention to it, not only during the first administration of the chloroform, but also throughout the operation, especially if it be attended with much bleeding. The pulse sometimes becomes intermittent or irregular during the administration of chloroform, more especially in elderly persons. This more commonly happens in the first exhibition of it, than when it is repeated during the course of an operation. I have not seen any harm from either of these conditions, but it is well to intermit the chloroform for ten or fifteen seconds, and let the patient have a few inspirations without it, if the pulse is not in a satisfactory condition. If the precaution be taken to ensure that the air the patient breathes shall never contain more than five per cent of vapour, the pulse can never be seriously affected by the direct action of the chloroform, and the state of the breathing affords the best warning against continuing the inhalation too long at a time.
The breathing is fortunately also a sign that cannot be [89/90] overlooked. It is by the breath that the chloroform enters, and it is extremely improbable that any one would go on giving the vapour after the breathing became stertorous and laboured.
The patient sometimes holds his breath after he is unconscious, and before he is insensible; this occurs under two conditions: first, after deep and rapid breathing, during which the patient seems to absorb more oxygen than is immediately required, under the circumstances; and in this condition, I have known him hold his breath for a whole minute, whilst the pulse was unaffected. The other condition in which the breathing is suspended, is when there is rigidity in the third degree of narcotism, and the respiratory muscles seem to partake of the general rigidity; the holding of the breath in these cases seldom continues so long as under the former circumstances. I do not consider that there is any danger from either of these kinds of suspension of breathing. I believe it always returns as soon as there is a want of oxygen in the system. Of course the inhaler need not be applied to the face when the patient is not breathing, and he may as well have an inspiration or two without chloroform when the breathing is renewed. It is seldom requisite to carry the effects of chloroform so far that the breathing becomes stertorous, and whenever stertor is observed, the inhalation should be suspended; under these circumstances, the patient is always insensible. In some cases, in which a little more chloroform has been inhaled than is necessary, the patient breathes for half a minute or so by the diaphragm only, and breathes in fact hardly at all. The abdomen rises and falls freely, but, from the muscles of the chest not fixing the ribs, hardly any air enters the lungs, and the face becomes rather livid; meanwhile the pulse goes on very well, and at last the patient draws a deep, sonorous inspiration, the face resumes [90/91] its proper colour, and all is right again. I have not heard of any accident from chloroform commencing in this manner. This state of breathing, when it does occur, usually takes place a few seconds after the inhalation has been left off, and arises from the accumulation of the effects of the chloroform, owing to the absorption into the system of the vapour which was contained in the lungs at the time when the inhalation was discontinued.44 This accumulation or increase of the effects of chloroform lasts for about twenty seconds; it is not dangerous unless the vapour is inhaled of too great strength, but it should be borne in mind in all cases. It may be prevented altogether, by reducing the strength of the vapour, just as the patient is getting insensible, or by giving it with intermissions of a few seconds, at this time.
The rigidity and struggling previously mentioned (pages 39 and 50) as occurring occasionally in the third degree of narcotism, more particularly in robust persons, often form a very prominent feature in the effects of chloroform; and have sometimes caused the medical man to discontinue the exhibition of chloroform, under the belief that it did not agree with the constitution of the patient, and that its further exhibition would be unsafe. The proper course to pursue is to continue the inhalation gently, till the struggling and rigidity are subdued. The patient is often insensible before these symptoms are subdued, but it is necessary to have him quiet, in order to enable the surgeon to operate with convenience and safety. I have always succeeded in subduing the involuntary struggling and rigidity, but have [91/92] occasionally occupied five or six minutes in doing so. It is desirable to proceed slowly and cautiously, because, when these symptoms occur, the patient has already absorbed nearly the usual quantity of chloroform, and he often holds his breath, and then takes a sudden and deep inspiration, when he might inhale an overdose of vapour, unless it were presented to him in a well diluted state.
When the rigidity and struggling are subdued, the breathing, in some cases, becomes stertorous, and relaxation of the muscles takes place, the limbs appearing quite flaccid; but by proceeding gently, these effects may generally be avoided, and the patient becomes quiet, whilst the breathing is natural, and the muscles are in a moderate state of tension. If the operator should be afraid to proceed with the exhibition of chloroform, on account of the violence of the muscular spasm and rigidity, it will be satisfactory to him to know that, if the inhalation is resumed in a few minutes, these symptoms will be less violent than at first.
Struggling and rigidity are less likely to occur, when chloroform is administered slowly, than under opposite circumstances; but it is impossible to prevent these phenomena altogether in certain patients. After they are once subdued, they but very rarely recur during the operation; the patient, in most cases, seems to take on, when he is subdued by the chloroform, the same relation to it that women, children, and persons in a state of debility have from the first. M. Chassaignac has called this condition one of tolerance of the chloroform. It is a condition in which the patient bears both the chloroform and the operation very comfortably; but tolerance of a medicine is generally meant to imply that the patient can take it in larger quantity than before. But this is the reverse of what occurs when the patient is in a tranquil state from chloroform; he has already absorbed a considerable quantity, which has most likely penetrated [92/93] deeply into the tissues, and he certainly does not require, and could not bear, so much as in the earlier stage of inhalation, where he is restless and breathing more quickly, and thus exhaling and getting rid of the chloroform at a greater rate.
It might be a question whether the absence of muscular excitement, in a number of cases, does not arise from the circumstance that anæsthesia, or absence of common sensibility, is obtained, and the operation performed, at a stage of narcotism anterior to that in which the muscular rigidity and spasm occur. This is true in a few cases, but I am satisfied by careful observation that, in the greater number of instances in which muscular excitement is absent, it would not occur at all, though the inhalation should be pushed to the most extreme degree. Many animals also are killed by chloroform without the least excitement of the muscular system occurring at any part of the process.
The pupils of the eyes are dilated in the deep state of insensibility which I have called the fourth degree of narcotism, but it is desirable to avoid carrying the effects of chloroform to this extent. They are occasionally dilated, however, under the slighter effects of chloroform, and even as the patient is recovering from its effects. In the third degree of narcotism, when the eyes are turned upwards, the pupils are usually, if not always, contracted; there seems to be a consentaneous action in the iris and the muscles which turn up the eye. The pupils seem also to be less sensitive to light, when the patient is insensible from chloroform, than at other times. This is all the information I am able to give about the pupils. Some writers have entered into a good deal of detail about the pupils, but their statements are very conflicting. The pupils are acted on by other causes, both external and internal, as well as the chloroform. The amount of light has great effect on them; and I have [93/94] seen them remain dilated for some time after the chloroform was discontinued, and then suddenly contract, as the patient began to use his eyes. Even if definite laws could be ascertained with regard to the action of chloroform on the pupils, in different doses, and under different conditions, there would be some difficulty in applying them during the administration of the vapour, as the patient cannot be made to direct his eyes to or from the light. There is also some difficulty in making correct observations on the pupils. Very often, when I am exhibiting chloroform, one of the bystanders lifts the patient's eyelid and makes a remark on the state of the pupil, and, on my looking in the face of the speaker, I often have occasion to tell him that his own pupils are quite as much dilated, or contracted, as the case may be.
With regard to the position of the eyes, they are usually turned upwards in the third degree of narcotism, as I have already said, but in a considerable number of instances they retain their usual position all through the inhalation. In a few cases, they are turned downwards, the pupils being almost hid under the lower eyelids, and causing a curious expression. I have noticed this most frequently in children of ten to fourteen years of age. I have scarcely ever seen temporary strabismus under the influence of chloroform.
The length of time which it is most desirable to occupy in the administration of chloroform, before the commencement of an operation, is about two minutes in infants, three minutes in children, and four or five minutes in adults. Circumstances occasionally occur, however, to lengthen these periods. The time during which the adult patient usually remains conscious whilst inhaling, is about two and a half minutes, but this period is sometimes prolonged from the nervousness of the patient, or his intolerance of the pungency of the vapour. Again, when unconsciousness [94/95] is induced, there is, in many cases, an increased flow of saliva; and although this usually causes no impediment, the patient sometimes keeps making efforts of deglutition which very much retard the inhalation; and, at other times, he holds his breath, with his mouth full of saliva, as if he had some obscure idea of disposing of it in a suitable manner.44 The delay which often arises from the struggling and rigidity has been already mentioned; but notwithstanding all these circumstances, it hardly ever takes more than seven or eight minutes to make a patient sufficiently insensible.
I have indeed met with a few cases in which a longer time has been occupied, but there has always been a physical reason for it. I have never had occasion to attribute the delay to any idiosyncracy, or great peculiarity in the patient, but only to the circumstance that the vapour did not enter the lungs in sufficient quantity within a given time. I have had under my care several patients who, it was supposed, were not susceptible of the effects of chloroform, or were, at least, very difficult to bring under its influence, as previous attempts had failed. It so happens, however, that I have had no difficulty whatever with any of these cases.
Two or three female patients who were about to undergo some trifling operation, preferred to leave off before they were unconscious, on account of unpleasant sensations in the head or chest, and to have the operation performed without the full effects of the chloroform; but there is no doubt the agent would have acted well enough if it had been continued.
The following case will show that chloroform may be in-[95/96]haled with advantage in cases which at first seem very unfavourable. I received a note in 1849 from a medical man in the country, in which he says:--"I have now a young lady under my charge, from whom I am about to remove a tumour attached to the ear. She is anxious to take chloroform, and by the desire of herself and mother, I yesterday administered it by way of trial, but only to what would be termed the second, and perhaps you would say, the first degree. She lost some sensation, but was quite conscious, and spoke. She felt giddy; there was tumultuous beating of the heart, and a much accelerated pulse, with a dilated pupil; a perfect coldness over the whole skin, with an equally cold perspiration; and, during recovery from this slight effect, severe tremors of the whole body, so much so as to shake the couch on which she was lying. From this state she did not recover for nearly an hour. She complained of great giddiness and oppression at her chest. She is a healthy looking, florid girl, but not strong, and has had, from time to time, severe spasm affecting her chest, so much so as to take away her breath. I have thus endeavoured to give you an outline of the constitution of my patient, how she had suffered, and what were the effects of the small dose of chloroform given by an inhaler. I never witnessed such extreme cold, tremor, or such tumultuous action of the heart; and am therefore anxious for the opinion of one who has administered chloroform under a greater variety of circumstances than myself, and to learn whether the symptoms I have described are sufficient to deter one from giving a sufficient dose to cause entire suspension of consciousness. My own impression is that they are sufficient to deter, but the patient and her friends being both anxious it should be inhaled if possible, I shall only be too glad to hear that you have witnessed like symptoms, and that you do not consider them sufficient indications of danger to deter me from its careful administration in the case." [96/97]
I advised that the chloroform should be administered again, and continued steadily till the patient should become insensible; expressing my belief that the unpleasant symptoms would subside as unconsciousness was induced. I received a reply to the effect that the operation had been performed very successfully under the influence of chloroform, although the vapour had an exciting effect for some time.
Repetition of Chloroform during an Operation. The first application of chloroform often suffices for an operation, if it be of short duration, without repeating the inhalation. In a few cases the patient remains insensible to the knife for three minutes after the inhalation is left off, but this is an exception; and one cannot, at all events, make sure of this prolonged effect of chloroform, without producing a deeper state of narcotism than is desirable. More usually, if the operation lasts more than a minute or two, it is necessary to repeat the inhalation; it is, indeed, generally desirable to let the patient have a few inspirations of air charged with chloroform vapour every half minute or so, whilst the operation continues, in order to keep up the insensibility. When the surgeon is cutting in the neighbourhood of important parts, it is desirable to prevent any sign of sensibility, and to keep repeating the chloroform so as to keep up the coma, without, however, causing embarrassment of the breathing, or wide dilatation of the pupil. In the greater number of operations, however, it is better to wait till there is some sign of sensibility, such as a slight cry or tendency to flinch, before the inhalation is resumed; and then a few inspirations of well diluted vapour make the patient quiet again.
As soon as a patient has ceased to inhale, the chloroform [97/98] begins to exhale in the form of vapour from the blood as it passes through the lungs. It cannot be detected by the sense of smell, after the lungs have been emptied, by two or three expirations, of the vapour they contained at the moment when the inhalation was discontinued; but I have detected it by chemical means, after consciousness had returned. The chloroform exhales in greatest quantity at first, and the patient usually recovers his sensibility and consciousness in the time which it ought to take for the chief part of the chloroform to be exhaled, according to mechanical principles; as will be explained in treating of the modus operandi of this agent. The last traces of the chloroform of course exhale more slowly, and a very minute and insignificant quantity may remain for a considerable period in the system, not only of the patient, but of anyone who was standing by whilst he inhaled.
It is probable that a small portion of chloroform passes out by other channels than that of the expired air: the latter, however, offers such a ready and expeditious outlet, that the quantity excreted in any other way is, most likely, very minute. I have on four occasions examined urine passed after the inhalation of chloroform, by boiling it in a flask, and passing the vapour, first through a red-hot tube, and afterwards through a tube moistened inside with solution of nitrate of silver, and I only on one occasion obtained a very slight precipitate of chloride of silver.
The patient usually becomes conscious within five minutes after the inhalation has been discontinued. After a short inhalation, for a very brief operation, consciousness sometimes returns immediately, and after a prolonged inhalation the recovery of consciousness is sometimes retarded till ten minutes have elapsed. Old people are often longer than others in awaking from the effects of chloroform, owing, no doubt, to their slower breathing and circulation. Chil-[98/99]dren, on the other hand, usually recover very quickly from its direct effects; but they often lapse into a natural sleep which lasts a considerable time--even for hours if they are not disturbed, and if the operation has left no painful wound or other cause of uneasiness.
It is desirable not to talk to the patient as he is recovering from the effects of chloroform, but to leave him to collect his ideas, and not speak to him till he is quite conscious, or makes some remark or inquiry himself. If not prevented by the medical attendant, the friends of the patient often address him the moment he opens his eyes; and the words they generally use are of a very equivocal meaning to one who cannot understand their application. They usually say "It's all over", which very often has the effect of raising an indefinite feeling of alarm in the patient; for, until he has had time to recover his memory, the operation he was to undergo is generally the farthest thing from his mind. When left to himself the patient usually recovers from the insensibility in a very tranquil manner. If he has not been moved whilst insensible, and awakes in the position in which he fell asleep, he supposes, very commonly, that he has not been asleep at all; and in a great number of instances will contend this point very stoutly, even after a protracted operation, and assert that the chloroform has not taken effect. It is as well to let him remain in this conceit for a while, or even till he finds out the mistake himself; for, if reminded of the pain they have been spared, just on waking after an operation, persons are liable to be excited by emotions of pleasure and gratitude; but a few minutes later, when the effects of the chloroform have more completely subsided, they are better able to control their emotions. A few persons wake with a full recollection of the preceding circumstances, and inquire if the operation is done; whilst others, on first [99/100] awaking, are still entirely occupied with the subject of their dreams.
The greater number of patients who inhale chloroform have to remain in bed on account of the operation which has been performed, but after minor operations, the patient is sometimes able to walk away within five minutes; although more frequently there is a little languor or feeling of fatigue for half an hour or so; and it is desirable in all cases for the patient to sit or lie quietly for this space of time, if not longer, before he makes any mental or bodily exertion, even if he feels quite well.
Sickness. The chief drawback to the benefits conferred by chloroform is the sickness which in many cases follows its use. It is most frequent when the inhalation takes place soon after a meal, and some of the precautions which are requisite in order to avoid this symptom, or render it as rare as possible, have already been described (p. 74); but it occurs in certain cases, notwithstanding the best measures which may be used for its prevention. Moving the patient as the effects of the chloroform are subsiding is very apt to excite vomiting when it might not otherwise occur; it is therefore desirable, when convenient, to allow the patient to lie for half an hour or so, without moving his head from the pillow. By this means, even when a feeling of nausea is present, it often subsides without the occurrence of vomiting. It is advisable also not to give the patient anything to eat or drink till about an hour after the inhalation, and, as a general rule, not even then, unless there is some inclination for it; for if anything is taken into the stomach before the effects of the chloroform have entirely subsided, it is apt to excite vomiting. Even medicine, such as an opiate, is better delayed for an hour or upwards, [100/101] unless there is an urgent necessity for giving it sooner. Severe faintness from loss of blood during an operation of course forms an exception to this rule; in such a case brandy and water should be given, and repeated if it should be vomited.
These rules respecting food are, moreover, meant to apply only to the use of chloroform in surgical operations, and not to its employment during labour. Under the latter circumstances, one allows the patient all the nourishment that is desirable, intermitting the inhalation now and then for the purpose. And chloroform, given in the moderate way in which it is employed in labour, hardly ever causes sickness, but often alleviates it when present from physiological causes.
The sickness induced by chloroform usually subsides of itself in the course of an hour, or even less; I, therefore, think it advisable not to do anything for it during this space of time. When it has continued beyond this period, I have found a little cold brandy and water to remove it in most cases; and when the tendency to vomit still remained after a few hours, I have seen it removed by a dose of opium. Effervescing draughts have not appeared to be of service in the sickness from chloroform, and sal volatile and draughts of warm water seem injurious. It is desirable for the patient to make no effort, but only to vomit if obliged to do so.
Several cases have come within my knowledge, in which the sickness has continued for two or three days after every thing that was taken into the stomach. These cases have not been under my care, but under that of the surgeon. I have been informed, however, that all the usual remedies for sickness were applied for the time mentioned above without success. The cases in which the sickness lasts so long form but a very small portion of the whole number in [101/102] which chloroform is administered, and they chiefly occur in persons who are subject to attacks of vomiting from slight causes, or, as they say, to bilious attacks.
The most usual time for the vomiting to commence is when the inhalation has been discontinued, and the effects of the chloroform are passing off. In many cases, it occurs before the patient has become quite conscious, and he does not know that it has occurred unless he is told. In a few cases, especially where there is a good deal of food in the stomach, the vomiting comes on before the operation is finished, or even before it is commenced. When vomiting comes on during an operation, it is apt to interfere with the inhalation, and it is sometimes difficult to prevent the patient from waking; but this can be accomplished by wiping the patient's mouth, and reapplying the chloroform, the moment the act of vomiting ceases. In many cases, however, the sickness does not come on till the patient is quite awake, and perhaps, even then, not until he moves. I believe that the sickness which is due to chloroform always commences within an hour or two, or at the farthest, just after the first food which is taken. I have known vomiting attributed to the chloroform which did not occur till the following day, but I ascertained that a dose of opium had been taken at night, and it was to this that the sickness was probably owing. In those cases where the chloroform does cause sickness in the first instance, it is not always the cause of all the vomiting which the patient may suffer. If the patient becomes infected or is inoculated with the poison of erysipelas or hospital gangrene at the time of the operation, he will probably be attacked with vomiting a day or two afterwards; and if sickness has already been caused by the chloroform, that which is due to disease may appear to be a continuation of it.
Soon after the introduction of chloroform, I administered [102/103] it to a gentleman, aged about 55, whilst a fatty tumour was removed from the nape of the neck. It did not turn out as fatty tumours usually do, but required to be dissected out. The patient had taken a meal before the operation, and vomited freely afterwards. On his visit the next morning, the surgeon thought his patient going on well. Vomiting returned, however, and the patient became affected with partial stupor and delirium, which his friends attributed to the chloroform. He became covered with an eruption of erysipelas over a great part of the body, had a very rapid pulse with great depression, and died on the fifth day. An examination after death showed that there had been diffuse cellular inflammation around the seat of the operation. A surgeon who assisted at the operation on the above patient, and also at the post mortem examination, removed an encysted tumour from the scalp of an old lady the day following the latter event. This operation was performed without chloroform, but the patient was attacked with erysipelas and diffuse cellular information, and died in three or four days.
Faintness and Depression. Although chloroform acts as a stimulant to the circulation, increasing the force and frequency of the pulse whilst it is being inhaled, it is occasionally followed by a feeling of faintness, especially if the patient remains in the sitting posture. At one period in the history of medical opinion, it would have been said that the depression was a consequence of the previous excitement. The facts, however, would not agree with such a doctrine. The subjects who are most stimulated by chloroform are the strong and robust, and they do not suffer from depression afterwards; whilst the feeble and debilitated, who are most liable to subsequent depression, are but little stimulated by it at the time of inhaling. Some amount of faintness and depression usually accompanies the sickness [103/104] caused by chloroform, and is in fact a consequence of it, being, like the sickness, most frequent after a full meal. This depression is usually relieved by vomiting. I have met with a few cases in which there has been more decided faintness, and once or twice absolute syncope after chloroform, which was not attributable to loss of blood. In these cases, however, the patients were in the sitting posture, and they recovered from the syncope immediately, on being placed horizontally. The patients most subject to faintness after chloroform are those who are subject to this affection at other times, being often persons in a state of anæmia, or having the symptoms of fatty degeneration of the heart. Faintness is, however, very much more rare after operations with chloroform than without it. The only cases in which I have seen it follow the use of chloroform in the horizontal position, and where there was no considerable loss of blood, have been two or three of operations on the rectum, performed before breakfast, and after a brisk purgative had been taken the previous night. It might be advisable, where persons in a state of debility have taken a purgative, to make an exception to the usual rule of prohibiting the breakfast, and to risk the inconvenience of vomiting rather than the more formidable symptoms of faintness from inanition.
The faintness which now and then follows an operation under chloroform should be treated on ordinary principles, as the horizontal posture, the application of the vapour of ammonia to the nostrils, and the exhibition of brandy or wine, if the other measures do not suffice. I never give ammonia internally where a patient is sick or faint, but the spirit of sal volatile, when at hand, serves very well to pour on the corner of a towel and apply to the nostrils.
Hysteria. I have already stated (p. 51) that chloroform occasionally excites hysteria in those who are subject to [104/105] that complaint; and that, in a few cases, the hysteria, which has been subdued by the chloroform, reappears as the effects of the vapour subside. It is nearly always in the female sex that one meets with these phenomena, although I have two or three times seen hysterical symptoms in the male for half an hour or so after the inhalation. The hysteria commonly takes the form of laughing or crying, but the patient sometimes remains quiet, and simply in an unconscious state. The hysterical symptoms usually pass off spontaneously, in half an hour or less, without any remedies; if they last longer, the ordinary remedies for hysteria may be applied. I am not aware that the hysteria has lasted longer than three or four hours in any of the cases in which I have administered chloroform, but it may have done so without my being informed of the circumstance. I was informed of the case of a young woman in King's College Hospital, who remained unconscious, or at least apparently so, for three days after chloroform had been administered for an operation, the nature of which I have forgotten. She recovered without ill effects. When the patient does not wake spontaneously, and cannot be roused to the waking state, within twenty minutes or half an hour after the inhalation of chloroform has been left off, we may rest assured that the patient is affected with hysteria--at least this has been the case in every instance with which have become acquainted. The physical properties of this agent do not permit it to remain long in the system, if the circulation and respiration are going on properly, and this circumstance ought to prevent unnecessary alarm, in the absence of other symptoms except the state of unconsciousness. I have, however, known great alarm to exist where the properties of chloroform were not well understood. Soon after its introduction, a medical man administered it to a young woman in domestic service, for the extraction of [105/106] a tooth. He became alarmed, in the first instance, from the impression that he had given an overdose. In a few minutes, however, the patient burst out in a loud fit of laughter, but again became unconscious, and various measures were used to restore her, including even artificial respiration, in the idea that she was still under the influence of chloroform. I was sent for thirty-six hours after the inhalation, and found the patient apparently in a profound state of insensibility, and breathing very feebly. Guided by the considerations mentioned above, I concluded that she was only labouring under hysteria, and that the anxiety of those about her tended very much to keep up the complaint. The anxious attendance on her was discontinued, she took some medicine containing valerian, and became quite conscious in few hours. I was told, however, that she did not seem quite well for some time.
I am not aware of any permanent ill effects having been produced by chloroform, although, amongst the multitudes of persons who have inhaled it, some have not failed to blame it for symptoms that have occurred afterwards.
A clergyman from the country called on me, in 1852, and the following are some notes I made when he left my room. He is 63 years of age. He said that he had inhaled chloroform about a year ago to have four teeth extracted. He felt very well for about a week afterwards, but on his pupils returning, and his beginning to apply himself to teaching, he became affected with flushings of the face and a rushing noise in his head, which lasted occasionally for a day or two, and have troubled him ever since. An eminent physician, whom he named, prescribed quinine, under the use of which he became worse. An eminent surgeon prescribed infusion of hops, etc., and he has tried other medicines without good effect. He had been recommended to travel, and had been to Switzerland; but the complaint troubled him when at leisure, as well as when ap-[106/107]plying himself mentally. He could not sleep at night, when affected with the attacks. He is rather deaf, and has been so for three or four years; he was also occasionally troubled with a rushing sound behind the ears before he inhaled the chloroform. He is rather short and rather stout, and has a florid complexion. The pulse was rather feeble. The second sound of the heart was rather louder than the first. In other respects its sounds were natural, but its impulse was not strong. In every respect, except the symptoms above named, the health of the patient was good, and he felt quite well between the attacks.
It was my opinion that the complaint of this gentleman was coming on long before he inhaled the chloroform, and that it depended on a much less transient cause. I have not heard from him since.
All narcotics are capable of causing death, and the discovery of preventing pain by inhalation consists essentially in carrying the effects of a narcotic much further than had previously been the custom; there was, therefore, every reason to apprehend that accidents might occur in the new practice, unless the effects of the medicines employed could be very effectually controlled. There are certain circumstances connected with the physiological properties of chloroform, as ascertained in the experiments previously related, which indicate how accidents may very easily happen with this agent, if not carefully and systematically managed. It was calculated (p. 74) that 18 minims of chloroform is the average quantity in the system of an adult, when sufficiently insensible for a surgical operation, and that this amount might be absorbed by the use of 36 minims, allowing one half of the quantity breathed to be exhaled again, without being absorbed; but 36 minims of chloroform make only 37.5 cubic inches of vapour, which, at the tem-[107/108]perature of 60° Fah., may exist in combination with 257 cubic inches of air, making it expand to not quite 300 cubic inches; the whole of which might be breathed in twelve ordinary inspirations of 25 cubic inches each. If the inhalation of vapour of this strength were continued till insensibility was induced, the lungs would still contain a great quantity of unabsorbed vapour. The amount of air usually present in the lungs is about 250 cubic inches, and if saturated with chloroform at the temperature of 60° it would contain the vapour of 30 minims. About half of this might be absorbed, the remaining half passing off in the expired air; but the addition of 15 minims to the 18 minims already absorbed would almost double the quantity of chloroform in the system, and bring the patient necessarily to the brink of death. It is true that, in the ordinary methods of inhalation, the air seldom becomes quite saturated with vapour, and usually is not more than half saturated, or accidents might be of much more frequent occurrence; but the above considerations are sufficient to show that the amount of vapour contained in the air breathed by the patient should not be left to mere accident, such as the varying temperature of the handkerchief from which the chloroform is breathed, or the greater or less extent of wetted surface over which the air passes. It should be recollected also that the patient sometimes draws a deep and sudden inspiration by which he may inspire 100 cubic inches of air, which would contain, if strongly charged with vapour, ten or twelve minims of chloroform--a large quantity to be suddenly added to that already in the circulation, when the patient is insensible, or nearly so.
It is, however, only by a knowledge of the different modes in which chloroform is capable of causing death, that the exact nature of the accidents from this agent can be understood, together with the means of preventing them, and [108/109] the reason why they are usually irremediable when they happen. If animals are kept for a very long time under the deep influence of chloroform, they become ultimately exhausted, the circulation and respiration are gradually weakened, and cease nearly together. Such a mode of death from this agent is never likely to occur to the human subject, and therefore need not engage our further attention. The following experiments illustrate the different modes of dying, when death is caused more suddenly by this agent.46
Experiment 23. A young but full-grown cat was placed in a glass jar, of the capacity of 1,600 cubic inches, and a fluid drachm of chloroform was introduced, by a portion at a time, through a tube in the cover of the jar. As twenty-five minims of chloroform produce twenty-six cubic inches of vapour, the atmosphere which the cat had to breathe contained nearly four per cent of vapour, and the jar was moved about, to ensure the uniform mixture of the vapour with the air. In five minutes, the cat became insensible, and lay breathing naturally. In about ten minutes more, the breathing became very feeble, and it ceased altogether in about another minute, or sixteen minutes after the cat commenced to breathe the chloroform. It was immediately taken out and laid on a table, and the stethoscope was applied to the chest. The heart could be heard beating distinctly at first, but the pulsations became slower and [109/110] feebler, and in about a minute they could be no longer heard. Just at this time, however, the cat took a gasping inspiration, and immediately the heart was heard to beat in a most rapid manner. The gasps were repeated, and the action of the heart became less rapid, but stronger. In a little time, both the breathing and the action of the heart became natural, the cat remaining, however, insensible for some minutes.
Experiment 24. A cat, about the same size as the last, was put into the same jar, and the same quantity of chloroform was introduced. It was removed at the end of four minutes, when it was so far insensible as to offer no resistance. Being laid on the table, it was made to breathe air charged with ten per cent of vapour of chloroform from a bladder. Twenty-five minims of chloroform were put into the bladder, which held 250 cubic inches, and it was filled up with the bellows. A portion of another bladder, which was attached to the stop-cock, was made to surround the head of the cat, which consequently breathed to and from the bladder. In half a minute it was quite insensible: in about half a minute more the breathing became difficult, and the sounds of the heart less distinct. The breathing became gradually slower, and ceased altogether between three and four minutes after the respiration from the bladder commenced. The sounds of the heart were rather frequent, and scarcely audible, just before the breathing ceased, and they could not be heard afterwards. The chest was opened three-quarters of an hour after death. The lungs were of a pale red colour, everywhere permeated with air and a small quantity of fluid blood flowed from them on making an incision. The right cavities of the heart were quite full of blood, and the left cavities contained a small quantity.
Experiment 25. A cat was made insensible in the same manner as the two previous ones. As it made strong efforts [110/111] to get out of the jar, and consequently breathed more deeply, the chloroform took effect sooner; and it was removed and laid on the table, in a passive state, at the end of two minutes and a half. The respiration and sounds of the heart were quite natural. The nose of the animal was placed in the mouth of a metal vessel, lined with bibulous paper, and used as a chloroform inhaler. The inhaler contained chloroform, and was surrounded with water of the temperature of 110° Fahr. The stethoscope was kept applied to the chest whilst the chloroform was exhibited. After four or five inspirations from the inhaler, the heart suddenly ceased to beat, the breathing still going on. The inhaler was removed as soon as I was satisfied that the action of the heart had ceased, and there were two or three rather convulsive respirations afterwards, and then the breathing stopped; but, between one and two minutes later, there were two or three feeble inspirations, accompanied with motion of the nostrils, but no returning action of the heart could be heard. The chest was opened ten minutes after death. The lungs were quite pale throughout. There was a little clear serum in the pericardium. The heart appeared quite motionless when first observed; but, after exposure to the air for a short time, there were some slight contractions of a few fibres of the right venticle. The right auricle and ventricle were filled with blood.
The air which this cat breathed must have contained much more than ten per cent of vapour.
In experiment 23 the breathing was arrested by the influence of the chloroform on the nervous centres, but the action of the heart continued, until it was stopped, or very nearly so, for want of respiration, as in asphyxia from privation of air. In experiments 24 and 25 the action of the heart was arrested by the direct effect of the chloroform; in one instance at the same moment as the respiration, and in the other instance, even before it. [111/112]
The paralysing effect on the heart of large doses of chloroform was shown in the first experiments which were made with this substance, viz., those by Dr. R. M. Glover in 1842. 47 In animals which were killed by injecting it into the jugular vein, the irritability of the heart was found to be destroyed, whilst this organ retained its irritability in those that were killed by the injection of chloroform into the arteries, stomach, or peritoneum. I have frequently arrested the action of the heart remaining in animals which were opened immediately after death, by blowing the vapour of chloroform on it; and I ascertained by some experiments on frogs, that the motion of the heart can be arrested by an amount of chloroform somewhat greater than suffices to suspend the respiration. As absorption of chloroform vapour is continued by the skin of these animals after the respiratory movements have ceased, they can be exposed to the vapour till the action of the heart is suspended by its direct influence.
Experiment 26. Four and a half grains of chloroform were introduced into a jar containing 600 cubic inches, being three-quarters of a grain to each 100 cubic inches, and, the vapour having been equally diffused, two frogs were put in. They tried to climb up the side of the jar, as if wishing to make their escape, and one or the other occasionally ceased to breathe for a minute or two, probably from disliking the vapour, but commenced to breathe again. In about five minutes the efforts to escape ceased, and they only moved to adjust their equilibrium when the jar was disturbed. They were now breathing regularly, and continued to do so till about ten minutes after their introduction, when all voluntary power ceased, and the breathing began to be performed only at intervals. They were allowed to remain till half an hour had elapsed, during the [112/113] last ten minutes of which time no respiratory movement was observed in either of them. On taking them out, and laying them on their backs, the pulsations of the heart were observed on each side of the sternum. These pulsations were the more distinct, from the lungs being apparently empty. I continued the experiment on these frogs, placing one of them back again, in the course of two or three minutes, in the same jar, with three grains of chloroform, and the other in a jar of 400 cubic inches capacity, with five grains. They were laid on their backs, and the heart of the former one, in air containing half a grain of chloroform to each 100 cubic inches, continued to beat distinctly and regularly, 45 times in the minute, for four hours that it remained in the jar, and it was not observed to breathe during the whole time, although it was watched almost constantly. The respiration commenced again within half an hour after its removal. In about an hour, it recovered its power of voluntary motion, and it was not injured by the long narcotism.
The pulsations of the heart of the other frog, in air containing a grain and a quarter of chloroform to each 100 cubic inches of air, became slower and more feeble, and in a quarter of an hour could not be observed. The frog was left in the jar a quarter of an hour longer, and removed when it had been in half an hour. The under part of the thorax was immediately opened sufficiently to expose the heart. It was moderately full of blood, but not contracting at all, and it did not evince the least irritability on being pricked, either at first or after exposure to the air for some time. It is evident that the heart of this last frog became paralysed by the absorption into the blood of more vapour, in addition to the quantity that was sufficient to arrest the respiration. The temperature of the room during this experiment was 65° Fah.
The effect of chloroform on the heart of the frog is further shewn by the next experiment.
Experiment 27. A frog was placed in the jar containing 600 cubic inches, with six grains of chloroform. In twenty minutes the respiration had ceased, but the heart continued to pulsate strongly. At the end of three-quarters of an hour, the pulsations were more feeble, and had diminished from 40 to 30 in the minute. An hour and five minutes from the commencement of the experiment, no movement of the heart could be observed. The frog was taken out of the vapour, and a portion of the sternum and integuments removed, so as partly to expose the heart, when it was found to be still contracting, with a very feeble undulatory motion. This motion increased in force, and, in a quarter of an hour after its removal, the heart was pulsating regularly and strongly, the ventricle apparently emptying itself perfectly. When the frog had been out twenty minutes, it was placed again in the same jar, with the same quantity of chloroform. In about ten minutes, the heart's action began to fail again; and in about twenty minutes, the slightest movement could no longer be perceived in it. The frog was immediately taken out, and the ventricle of the heart was pricked with a needle. In a few seconds, a slight quivering was observed,--whether the result of the prick is not certain,--and the action of the heart became gradually reestablished as before. It was arrested a third time by exposure to the vapour; and although, in its third removal, the anterior extremities of the frog had become rigid, the heart resumed its action partially, and continued to contract feebly for three or four hours after the rigidity of death had invaded the body and limbs of the animal. The temperature of the room was 62? during this experiment.48
In the human being and all other creatures of warm [114/115] blood, any vapour which is inhaled and absorbed in the lungs passes at once to the left side of the heart, and as the coronary arteries are the first branches given off from the aorta, the heart must, during the process of inhalation, be always a very little in advance of the rest of the body, as regards the amount of vapour to which it is subjected. This, however, is no source of danger, as regards chloroform, if the inhalation takes place in a gradual and uniform manner; for the heart being able, as shown by the above experiments on frogs, to bear a greater amount of this narcotic than the brain, its action continues even after respiration has ceased, if the vapour is added only by a little at once to the blood, as it passes through the lungs. But if the air which the patient breathes be too highly charged with vapour, it is easy to understand how the sensibility of the nerves of the heart may be paralysed, notwithstanding their power to bear somewhat more of this agent than the brain and nerves of respiration. I calculated (p.74) the quantity of chloroform which would suffice to arrest respiration in the adult of average size to be thirty-six minims, provided it were equally diffused through the circulation; but supposing a patient breathes, at any time, air containing ten per cent of vapour of chloroform, a considerable part of this might enter the lungs at a very few inspirations, for thirty-six minims of chloroform occupy only 37.5 cubic inches, and would be contained in 375 cubic inches of air, and might be breathed in less than a minute; but for the whole of the blood to pass through the lungs occupies a considerable time--I believe about four minutes in the adult--and therefore the portion of blood which is passing through the lungs, at the time when vapour of the above strength is inhaled, must become much overcharged with chloroform, making every allowance for the portion of vapour which is expired again, without being absorbed. [115/116]
I have observed the manner in which the breathing and circulation ceased in a great number of instances, with the stethoscope applied to the chest of the animal, when the quantity of chloroform contained in the air it breathed was known, and have notes of the result. The animals were chiefly cats, which would otherwise have been killed by prussic acid, or in some other way. In every instance in which the quantity of vapour in the air breathed by the animals was from three to six per cent, the respiration ceased whilst the sounds of the heart were still very distinct, as in Experiment 23, related above; in many instances the heart continued to beat from two to three minutes after the breathing had ceased, and, in a great number of instances, there were one or more gasping inspirations just at the moment when the sounds of the heart ceased. In many cases these gasping inspirations caused the action of the heart to return, as in Experiment 23, if the animal had been withdrawn from the chloroform; but this was not always the case; and if the chloroform was still breathed during these gasping efforts, all signs of life immediately ceased in every instance.
When, on the other hand, the air breathed by the animals contained eight or ten per cent, or upwards, of vapour of chloroform, the action of the heart was always seriously affected and rendered extremely feeble, if it did not actually cease, at the time the breathing was arrested. In several instances, indeed, the sounds of the heart entirely ceased before the breathing, as in Experiment 25; and although the chloroform was withdrawn, in this and many other experiments, the moment the heart ceased to beat, and fresh air was drawn in by inspiratory efforts, it very rarely had the effect of restoring the heart's action, although this happened so frequently when that organ had gradually ceased to act on account of suspension of the breathing, by the effect of more diluted vapour. [116/117]
In order to see more precisely the action of the vapour of chloroform on the heart, when not sufficiently diluted, the chest and pericardium were opened on four occasions, in cats and a rabbit, and chloroform was exhibited by artificial respiration. I was assisted by Mr. Peter Marshall in these experiments, and the following is the account of one of them.49
Experiment 28. A young rabbit, rather more than half-grown, was made insensible by breathing air charged with four per cent of vapour of chloroform in a large jar. The trachea was then opened, and a tube was introduced and tied. The lungs and heart were then exposed, by making an incision and removing the lower half of the sternum, with the adjoining part of the cartilages of the ribs on each side. The front of the pericardium was also cut away, to expose the heart. Whilst these operations were performed, artificial respiration was kept up by means of a bladder of air attached to the tube in the trachea. The heart contracted vigorously and quickly, and the lungs were of a light red colour. The rabbit was beginning to show signs of returning sensibility, when the bladder of air was changed for one containing ten per cent of vapour of chloroform. The bladder contained 125 cubic inches, and twelve minims of chloroform were put in before it was filled with the bellows. Three or four inflations of the lungs only were made, when I perceived that the heart was beginning to be affected, and I changed the chloroform for a bladder containing only air. These three or four inflations of the lungs with chloroform, had the effect of causing the right cavities of the heart to become distended with blood, and its pulsations to become much slower. In two or three minutes, however, the action of the heart was quite reestablished by the artificial respiration, the pulsations being vigorous and [117/118] frequent, and the ventricles being apparently emptied at each contraction. The bladder charged with ten per cent of chloroform was again attached, and artificial respiration was made with it. The right ventricle began almost immediately to become distended; and, by the time that eight or ten inflations of the lungs had been made, the contractions of the heart were very slow and feeble. Artificial respiration with air was resumed, but without the effect of restoring the action of the heart. The lungs were observed at the time when the right ventricle was becoming distended, and it was noticed that their colour was unchanged. They afterwards became paler, as the artificial respiration was continued after the ventricle had ceased to empty itself. No contractions of the diaphragm were observed after the first inflation of the lungs with chloroform, and the rabbit did not gasp at any time; whilst the cats were observed to make a few gasping efforts at the time when the heart's action was ceasing.
The circumstance of the lungs not changing in colour at the moment when the right ventricle was becoming distended, which was observed in the cats as well as in the rabbit, shows that the distension arose from the failure of the contractile power of the heart, and not from impediment to the pulmonary circulation; for, in the latter case, the lungs would have become congested, and of a deeper colour. In one of the cats, it appeared to me that the left, as well as the right ventricle, was distended with blood; but this distension of the left ventricle did not continue.
In the Experiments 24 and 25, related above, the animals were first made insensible by vapour of moderate strength, in order to keep them quiet for the application of the stethoscope whilst the stronger vapour was inhaled, but when animals are made to breathe air containing ten per cent or so of vapour of chloroform from the first, death takes place [118/119] in the same manner, i.e. by the direct action of the chloroform on the heart. Under these circumstances the creatures die suddenly, after a brief interval of agitation and excitement, without previous insensibility. This is what has happened in some of the accidents from chloroform, to be related further on; whilst in many cases death has happened after a longer or shorter period of insensibility.
In many of the fatal cases of inhalation of chloroform the alarming symptoms commenced whilst the patient was still inhaling, but in a considerable number there was no sign of danger until after the inhalation had been left off; and this is a result which may be imitated on animals. The two following experiments, which were made at Dr. Sibson's on December 27th, 1849, illustrate this point.
Experiment 29. The subject of this experiment was a young guineapig, about half grown. Ten or twelve drops of chloroform were put into a short bent metal tube, lined with bibulous paper, which formed part of an inhaler, and one end of the tube was applied to the animal's nose, which closed it. The guineapig consequently breathed backwards and forwards through the tube, which was, moreover, warm from being held in the hand. It struggled at first, endeavouring to get away from Dr. Sibson, who held it; but in twenty or thirty seconds it became quiet; and observing that the conjunctiva was insensible, I withdrew the chloroform, and the guineapig was laid on the table. We remarked that the breathing was very slow; and scarcely had this remark been made, when it ceased altogether, three or four inspirations only having been made since the inhalation was left off. Dr. Sibson proceeded immediately to open the body; but as soon as he had divided the integuments of the chest the animal began to make some convulsive gasping inspirations, during which the mouth was widely opened, and we observed that the diaphragm acted alone, the ribs [119/120] being pressed inwards by the atmosphere. The heart was not contracting at all when the pericardium was first opened; but in a few moments the auricles began to contract rhythmically. The lungs were of a light red colour.
Experiment 30. Another guineapig of the same age was treated in the same manner, except that I removed the tube from the nose for a short time between every two or three inspirations, in order to see if I could not make it insensible in this way without a fatal result. In half a minute or so the animal no longer required to be held, but lay on the table without making any resistance, the conjunctiva being still sensible, and some motion of the limbs, apparently voluntary, remaining. It only inhaled once after Dr. Sibson ceased to hold it, and whilst in the state just described, and then only for two or three inspirations. After this it appeared quite insensible, and no more chloroform was given.
It breathed at first naturally, except more slowly and gently than before the inhalation; but the breathing became slower, and ceased altogether about a quarter of a minute after the inhalation had been left off. The body was opened immediately. When the pericardium was opened, the auricles were observed to contract slightly, and the contractions increased after their exposure to the air.
The amount of vapour in the air breathed by these two guineapigs is not known, but there is no doubt that it was upwards of eight per cent.
If it were possible for a medical man to mistake or disregard the symptoms of approaching danger, and to go on exhibiting vapour of chloroform, diluted to a proper strength, till the death of the patient, this event would take place slowly and gradually, as in Experiment 23, related above, [120/121] and every other experiment in which the air did not contain more than five per cent of vapour. The action of the heart would survive the respiration; there would be a great tendency to spontaneous recovery, and the patient would be easily restored by artificial respiration, if it were performed whilst the heart was still acting; as I have always found it to be successful in animals under these circumstances.
In examining the recorded cases of fatal inhalation of chloroform, we shall find, however, that they have none of them taken place in this gradual manner; but that in all cases the fatal symptoms, if not the actual death, have come on very suddenly. Dr. Sibson was, I believe, the first to point out that, in the fatal cases of inhalation of chloroform, death was caused by its paralysing the heart; but he was not at that time aware of the physical conditions under which this agent may act directly on the heart. In commenting on the first four deaths from chloroform, he says:50 "In all the four cases it is manifest that the immediate cause of the instantaneous death lay in the heart. The heart, influenced by the poison, ceased to contract, not from the cessation of respiration, for the heart in asphyxia will beat from one to three minutes after respiration has ceased, but from immediate death of the heart. There is no doubt a combination of causes operating to destroy the heart's contractile power: the mental influence, the congestion in the systemic, and that in the pulmonary capillaries, will all have a material influence." And further on he says: "We are obliged, then, from the experience of these cases, to conclude, that in man the death is usually instantaneous, and due, as every instantaneous death is, to paralysis of the heart. In animals the death is usually due to paralysis of the muscles of respiration. It is chiefly owing to the [121/122] superior control of the mind over the body in man, that in him the poison acts on the heart more than in dogs."
I had been long aware that chloroform was capable of paralysing the heart in animals; and, indeed, that sulphuric ether would do so when it could reach the heart in sufficient quantity;51 and soon after Dr. Sibson's remarks I was able to ascertain and point out the strength of the vapour which will produce this effect, and how one may avoid the risk of it, by having the vapour sufficiently diluted.51a The greater number of experimenters who have killed animals with chloroform have found that the action of the heart continued after the breathing ceased; but they did not either control or ascertain the proportion which the vapours of chloroform bore to the inspired air. In Mr. Thomas Wakley's experiments the action of the heart continued after the breathing had ceased; and this was the case in a great number of experiments performed by a Commission which reported to the Society of Emulation of Paris, in 1855.52
This Commission came to the conclusion that, in all instances in which animals are killed by chloroform, the action of the heart survives the respiration; but they might have administered chloroform to an equal number of human patients without any one of them being cut off by sudden paralysis of the heart. If animals were usually to die suddenly of paralysis of the heart, when the chloroform is given in a manner similar to what may be called its ordinary administration to patients, we should be at a loss to know how this agent could be used at all. It is only reasonable to suppose that, in experiments so conducted, that mode of death should usually be met with which would occur to the [122/123] human subject, if the chloroform were continued, in the disregard of dangerous symptoms, till death should ensue. I have, indeed, been informed of several instances in which animals died in a sudden, and what was thought an unaccountable manner, whilst chloroform was given to prevent the pain and struggles which would be occasioned by physiological experiments. In these cases there is no doubt the heart was paralysed; but the experimenters were often too intent on other matters to observe the circumstance. By a proper arrangement of circumstances, however, one may produce at will the event in animals which occurs, in fact, so very rarely to a patient, although it may at any time happen if great caution, guided also by right principle, is not used.
Air, when saturated only at 60° Fah., contains 12 per cent of vapour of chloroform, and at 70° 19 per cent (p. 33); and 8 or 10 per cent in the inspired air is capable, as we have seen, of causing sudden death by paralysing the heart; but in practice the air is usually far from being saturated, in passing over a handkerchief or similar material, even at the temperature at which it is inhaled; and this is generally lowered considerably by the absorption of caloric by the chloroform, as it changes its condition from a liquid to a vapour. Moreover, air strongly charged with vapour of chloroform is not easy to breathe, owing to its pungency; and the physiological knowledge and close attention of every medical man who administers this medicine causes him to withdraw it immediately on the least appearance of danger.
Case 1. The first death from chloroform was that of Hannah Greener, which occurred at Winlaton, near Newcastle, on the 28th of January, 1848. The patient was a girl of 15, who required to have the nail of the great toe [123/124] removed. A similar operation had been performed on the other foot, in the previous November, in the Newcastle Infirmary, when ether was administered with a satisfactory result. The following is the account of the accident by Dr. Meggison, who administered the chloroform: "She appeared to dread the operation, and fretted a good deal: in fact, she commenced sobbing on our entering the house, and continued so until seated in the operating chair, and commencing the inhalation, which was done from a handkerchief on which a teaspoonful of chloroform had been poured. After drawing her breath twice, she pulled my hand from her mouth. I told her to put her hands on her knees, and breathe quietly, which she did. In about half a minute, seeing no change in breathing, or alteration of pulse, I lifted her arm, which I found rigid. I looked at the pupil and pinched her cheek, and, finding her insensible, requested Mr. Lloyd to begin the operation. At the termination of the semilunar incision she gave a kick or twitch, which caused me to think the chloroform had not sufficient effect. I was proceeding to apply more to the handkerchief, when her lips, which had been previously of a good colour, became suddenly blanched, and she spluttered at the mouth, as if in epilepsy. I threw down the handkerchief, dashed cold water in her face, and gave her some internally, followed by brandy, without, however, the least effect, not the slightest attempt at a rally being made. We laid her on the floor, opened a vein in her arm, and the jugular vein, but no blood flowed. The whole process of inhalation, operation, venesection, and death, could not, I should say, have occupied more than two minutes." 53
An examination of the body was made the day after death by Sir John Fife and Dr. Glover, who reported as follows:--"The body was that of a well-grown female of [124/125] about fifteen years of age.... On opening the chest, the lungs were not collapsed. One or two very slight adhesions were encountered on separating them from the walls of the chest. The external appearance of both lungs, over the whole surface, but especially in the inferior portions, was that of organs in a very high state of congestion. They were mottled with patches of a deep purple, blueish, or scarlet hue. They were everywhere crepitant. Along the outer and interior border of both lungs, particularly of the upper lobe of the left lung, were several emphysematous bubbles of small size. . . . The pulmonary tissue was filled with bloody froth, which was also found in the interior of the bronchi, mixed with mucus. There was no appearance of hepatization. On examining the larynx and trachea, the epiglottis was found reddened at the summit, of a vermilion hue. The mucous membrane of the larynx was redder than natural--mottled with vascular patches. The sinuses of the larynx contained a good deal of dark mucus. The œsophagus was healthy. The stomach was distended with food. Some of the veins were more distinct than usual. The heart contained dark fluid blood in both its cavities: very little in the left. Its structure, and that of the great vessels near it, quite healthy. The brain, externally and internally, was more congested than usual; and the ventricles contained rather more than the usual quantity of serum."54
Sir John Fife and Dr. Glover expressed the opinion that chloroform caused death by producing congestion of the lungs. After the further experience which has been gained respecting chloroform, this opinion of the mode in which it caused death, in the above case, would probably not now be offered. Indeed, in similar cases which have since occurred, the same opinion has not been advanced; [125/126] and as the lungs were crepitant throughout, in the above case, it is probable that the congestion was not greater than is commonly met with in cases of sudden death without hæmorrhage. Dr. Simpson published his opinion, immediately after this case occurred, that it was not caused by the chloroform, but by the brandy which was given when the alarming symptoms came on; but Dr. Meggison replied that only a teaspoonful of brandy was given; that it was swallowed, though with difficulty; that there were no symptoms of choking from it; and that the girl was without pulse when it was given.55
From the lips becoming suddenly blanched in the above case, there is every reason to conclude that the heart was suddenly paralysed. The patient breathed for a little time after this, and was able to swallow, though with difficulty. The process of inhalation occupied only a little more than half a minute in Dr. Meggison's estimation; yet he appeared to think that the fluid drachm of chloroform which he had put on the handkerchief had evaporated; for he was about to apply more when the alarming symptoms appeared. But supposing only one-third of the drachm was actually inhaled into the lungs in the half minute, the vapour would necessarily be in a highly concentrated state--probably twenty cubic inches of vapour in 200 cubic inches of air, which would be adequate to occasion the result which happened. In the short space of about half a minute, the blood could not be uniformly impregnated with the vapour; only a portion of it could pass through the lungs in the time; yet, as the patient was rendered insensible, this portion must necessarily have been highly charged with vapour.
It was often the practice to render the patient insensible in as short a time as half a minute, when chloroform was first introduced, but I believe never without danger; and I [126/127] had expressed the opinion before any accident happened, that, for reasons such as I have stated above, a patient should on no account be rendered insensible in less than two minutes. 56
Case 2. The next recorded case in which the inhalation of chloroform was fatal, occurred at Cincinnati, on the 23rd of February, 1848. The subject of it, Mrs. Martha G. Simmons, was thirty-five years of age, and enjoyed good general health; she was the mother of six children, and her last confinement occurred eight weeks before her death. The patient exhibited no alarm on account of inhaling the chloroform, which was administered by two dentists, who were not members of the medical profession. It was breathed from an inhaler which Dr. Morton of Boston contrived for sulphuric ether. This inhaler consisted of a glass globe four inches and a half in diameter, and contained a sponge about one-third filling the globe, and saturated with chloroform.
Two female friends of the patient reported the following as the events which occurred. "The respiratory movements appeared to be free; chest heaving. While inhaling, the face became pale. At the expiration of about one minute, the instruments were applied, and four roots of teeth extracted. The patient groaned and manifested what they regarded as evidences of pain, while the teeth were being extracted, although she did not speak or exhibit any other sign of consciousness. As the last root came out, which was about two minutes from the beginning of the inhalation, the patient's head turned to one side, the arms became slightly rigid, and the body drawn somewhat backwards, with a tendency to slide out of the operating chair. At this instant, Mrs. Pearson states that she placed her finger [127/128] upon the patient's pulse; observed that it was feeble, and immediately ceased to beat; respiration also ceased about the same time. The face, which was previously pale, now became livid, as did also the finger nails; and the lower jaw dropped, and the tongue projected a little at one corner of the mouth, and the arms were perfectly relaxed. The females regarded her as being then quite dead." 56a
The dentists gave nearly the same account, saying that the breathing was at first slow, and that the patient inhaled twelve or fifteen times, occupying from a minute to seventy-five seconds. They committed the great error of not placing the patient at once in the horizontal position, when the alarming symptoms came on, but kept her sitting in the chair, from five to ten minutes, whilst they sent out for restoratives. They thought the patient was living during this time, but her female friends thought not. The patient was placed on a sofa, and sometime afterwards artificial respiration and galvanism were applied without effect.
An examination of the body was made twenty-six hours after death by Drs. Mussey, Lawson, Baker and Mulford. The following are the chief particulars of the appearances met with. A larger quantity of blood than usual flowed from the sinuses of the dura mater. General aspect, colour, and consistence of the brain, normal. Lungs considerably but not intensely congested; crepitated freely at all points; no extravasation. Lining membrane of bronchia slightly congested, apparently the result of recent catarrh; deeply stained by the blood. Pleura at all points highly injected; six drachms of bloody serum in the right, and two ounces in the left chest. Pericardium contained six drachms of bloody serum. Heart flaccid, and all its cavities entirely empty; inner surface of both ventricles and auricles deeply [128/129] stained. Abdomen--one ounce and a half of bloody serum in the right hypochondrium. Stomach and intestines distended with gas. Partially digested aliment, amounting to about three gills in the stomach. Blood fluid as water in every part of the body; not a coagulum was seen in any vessel. Lining membrane of all the bloodvessels deeply stained. The colour in every part of the system was that of ark venous blood.
It was estimated, in the inquiry which took place respecting this case, that one-fourth part by measure of what the patient inhaled might be vapour of chloroform; but this is evidently an over-calculation, for there could not be this quantity unless the interior of the glass globe were maintained at the temperature of 80° Fah. and the air were quite saturated with vapour in passing through it; however, less than half the amount of vapour here assumed would have the effect of causing sudden death, in the way it happened. The period of the inhalation, a minute or seventy-five seconds, during which the patient took twelve or fifteen inspirations, did not admit of the blood in the body being regularly and uniformly charged with the chloroform; and the increase of its effects, owing, no doubt, to the absorption and circulation of the vapour contained in the lungs at the moment when the inhalation was discontinued, was well marked. The patient became pale during the inhalation, but the alarming symptoms suddenly came on during the extraction of the fourth stump, probably within half a minute after the inhalation ceased. The patient seemed, in fact, to die with the slight struggle that took place at this moment. In the case of Hannah Greener, related above, the spasm at the moment of dying was even more marked. This is a symptom I have often seen during the death of animals killed suddenly with vapour of chloroform in a concentrated state, before they were made thoroughly insensi-[129/130]ble. Although the heart was empty, the stained condition of its cavities showed that they had contained blood at the time of death and afterwards. Owing to its fluid state, it probably escaped from the heart during the moving of the body; especially during the examination of the head, which was made first.
Case 3. The next recorded case of death from chloroform is reported by Dr. John C. Warren, of Boston, U.S., in the London Medical Gazette.57 His report, apparently extracted from some other report, is as follows.
"Name--Patrick Coyle. (Age--not stated.) Date--March 1848. Disease--fistula. Previous use of chloroform--once. Time of inhalation--about one minute. Quantity consumed--about thirty drops (Query minims.) Posture--upon the side. Lapse of time till death--about one minute. Symptoms--showed signs of pain, by putting his hand to the part; in a moment his pulse, which was full and natural, sank: death. Morbid appearances--brain, with membranes, natural and healthy. Heart enlarged, pale, and soft; two or three ounces of serum in pericardium; bloodvessels with dark fluid blood. Lungs, studded with tubercles; abscess in each; lower parts congested; pleura extensively adherent; stomach--mucous membrane softened, its veins turgid."
Nothing is said about the apparatus used in this case, but from the summing-up of Dr. Warren's paper, it must have been either a towel or a handkerchief. The quantity of chloroform employed appears to have been much less than in the two previous cases. In speaking of drops, the writer probably means minims, or what is the same, a quantity equal to as many drops of water. Thirty drops of chloroform from a small phial are only equal to between six and [130/131] seven minims, and if they were dropped on a handkerchief, so that they might be counted, they would evaporate entirely during the process. Supposing the quantity used to have been what is probably meant--half a fluid drachm--it would be quite adequate, according to the calculations previously made in these pages, to cause the accident which happened. The period of inhalation was again very short--one minute; and the evidence of paralysis of the heart is distinct:--"In a moment his pulse, which was full and natural, sank: death."
Case 4 was that of Maddle. Stock, aged thirty, and occurred at Boulogne, in May 1848. The operation was that of opening a sinus in the thigh, between two and three inches in length, at the bottom of which a small splinter of wood was found. M. Gorré, the surgeon who attended the patient, says: "I placed over the nostrils of the patient a handkerchief moistened with fifteen to twenty drops of chloroform at most." It is necessary to remark, however, that a judicial examination of the bottle from which it had been taken, proved that from five to eight grammes had been used, a quantity equal to from 77 to 123 grains, and there are three drops of chloroform to a grain. M. Gorré proceeds to say: "Scarcely had she taken several inspirations, when she put her hand on the handkerchief to withdraw it, and cried with a plaintive voice, 'I choke.' Immediately the face became pale; the countenance changed; the breathing embarrassed; and she foamed at the mouth. At the same instant (and certainly less than a minute after the beginning of the inhalation), the handkerchief moistened with chloroform was withdrawn." M. Gorré performed the operation, but he expressed the opinion afterwards that death had already taken place when he made the incision. Amongst the means used, with a view to resuscitate the [131/132] patient, was inflation of the lungs, which was performed with such force as to produce permanent dilatation of the air-cells. The lungs, besides being distended from this cause, were found after death to be visibly engorged in their lower lobes. When cut into, a large quantity of black blood escaped. The cavities of the heart were empty, but the internal membrane, especially of the right cavities, was red. The tissue of the heart was pale, and was easily torn. Air was found in the pulmonary veins, and in most of the systemic veins throughout the body. The blood was very dark-coloured and fluid. 58
M. Gorré reported the above case to the Academy of Medicine of Paris, and a commission was appointed to inquire and report on it, who came to the following conclusions.
"1. In the medico-legal fact submitted to our notice, we found no indication of the poisonous action of chloroform; and consequently we reply to the minister, that the patient of M. Gorré did not die from the effect of inhalation of that agent.
"2. There have occurred a great number of analogous cases of sudden and unforeseen death, during operations, without any administration of chloroform, in which the most minute examinations have failed in detecting any assignable cause of death.
"3. In the case in question, the most probable cause, under all circumstances, seems to have been the mixture of a considerable quantity of gas with the blood. 59
The report on this case gave rise to frequent discussions in the Academy, extending over several months, and the Academy ultimately confirmed the above conclusions, but [132/133] not without considerable opposition from M. Blandin, M. Jules Guérin, and other members.
M. Malgaigne, the reporter to the commission, and others, who strongly supported the first of the above propositions, founded their argument chiefly on the assertion that chloroform always produces intoxication and insensibility before death; but this is incorrect, as I have explained above; and I took occasion to make the following remarks on this point about the time when the discussion in the Academy of Medicine took place. I said: "I have several times made animals--small birds, mice and rabbits--breathe air saturated with vapour of chloroform at the temperature of the atmosphere, and the consequence has always been that, after attempting for a few seconds to escape from the capacious jar in which they were enclosed, they suddenly exhibited signs of distress, and died without any interval of intoxication or insensibility, in periods varying from less than half a minute to a minute after their first exposure to the vapour." 60
The power of chloroform to cause sudden death without previous insensibility is now, I believe, generally admitted. The French call this kind of fatal action sideration.
With regard to the second conclusion of the commission, if it had been really true that the surgeon put only fifteen to twenty drops at the most of chloroform on the handkerchief, one would have been inclined to admit it; but with the quantity actually employed, and the strong sensation of choking it occasioned just before death, one must, in connection with other cases, and with what is known of the action of chloroform, attribute the fatal event to this agent, rather than to the surgical operation, which was not of a serious nature.
With regard to the third of the above conclusions, it is [133/134] not a little remarkable that most even of those speakers who opposed the conclusions of the commission, agreed that death was caused by a sudden development of air in the veins; and differed from them only in this, that they consider the chloroform as the cause of the evolution of air or gas, and that it proved fatal in this way. That the air was not caused by putrefaction, and that it did not enter by the wound in the thigh, may be readily admitted, but there remains the artificial respiration, which was performed with such force as to produce permanent dilatation of the air-cells. It was argued in the Academy that, as the air was in the systemic, as well as in the pulmonary veins, it could not have been introduced by the artificial respiration, since the left ventricle had previously ceased to act; but the action of the left ventricle is not necessary for the passage of the contents of the arteries through the capillaries into the veins, since this commonly goes on after death, the arteries being usually found entirely empty of the blood they must have contained at the moment of death.
With regard to the passage of the air out of the heart into the arteries, supposing that the pulmonary veins were ruptured during the inflation of the lungs, there is an observation of Dr. Sibson's which will explain both this circumstance and the fact of the heart itself being found empty of blood. He found that the heart was often emptied of blood by distending the lungs with air after death in preparing the body for diagrams of the position of the viscera.61
With the conclusions above quoted, some additional ones were adopted from the second part of the report of the commissioners; in these it was admitted that chloroform is capable of causing death, if administered too long, or in too large doses. One of these additional conclusions, however, is as erroneous as the previous ones. It is, "there is risk of [134/135] asphyxia when the anæsthetic vapour is not sufficiently diluted with air." When the vapour is not sufficiently diluted with air, the risk is one of sudden death, by paralysis of the heart. Chloroform does not yield enough vapour, at the natural temperature and pressure of the atmosphere, to exclude the air to the extent which would cause asphyxia. When chloroform vapour largely diluted with air is long continued, it may cause, not real asphyxia, but a mode of death resembling it, owing to the medulla oblongata and nerves of respiration becoming over narotised.
Case 5 is that of a young woman at Hyderabad, who inhaled chloroform to undergo amputation of the middle finger. A drachm was sprinkled on a handkerchief and inhaled. The operator described what occurred as follows: "She coughed a little, and then gave a few convulsive movements. When these subsided, I performed the necessary incisions, which of course did not occupy more than a few seconds. Scarcely a drop of blood escaped." The absence of bleeding seemed to be the circumstance which called the attention of the operator to the state of his patient; and after describing the means which were used without avail to bring about recovery, he continues, "I am inclined to think that death was almost instantaneous; for, after the convulsive movements above described, she never moved or exhibited the smallest sign of life."62
Case 6. Charles Desnoyers, aged twenty-two, a patient in the Hôtel-Dieu at Lyons, affected with scrofulous disease of the left wrist, having to undergo transcurrent cauterisa-[135/136] tion of the joint, inhaled chloroform from an apparatus for five minutes, and died at the beginning of the operation.63 Further particulars are not given.
Case 7. A young gentleman, who had returned from Australia to visit his relatives in the neighbourhood of Govan, inhaled chloroform for an intended operation on the great toe, in December 1848. It is stated that the patient, after inhaling it, almost instantly expired. This account appeared in the Glasgow Herald, and was copied into the medical journals.64 I believe that no further account of the case was ever published.
Case 8 occurred on January 19th, 1849. It is related by Dr. John C. Warren.64a John Griffith, an Irishman, aged thirty-one, a seaman in the American navy, was admitted into the New York Hospital early in December 1848, on his return from Mexico. He was suffering with diarrhœa, chancres, and hæmorrhoids. The following is the account of this accident.
"Gurdon Buck, jun., attending surgeon to the New York Hospital, being sworn, says, that on or about the 26th of December, I advised that chloroform should be administered to the deceased, for the purpose of examining the condition of the rectum, the parts being in such a state of excessive irritation as scarcely to admit of a separation of the nates. The patient recovered from the effects of the chloroform, and remained in all respects in the same condition, except the local ailments spoken of; and he having never complained of either his head or his chest, and not having suffered from the first administration of chloroform, I directed it to be administered to him for the purpose of performing [136/137] an operation upon the rectum, and the operation of circumcision to remove a phymosis caused by the chancres: the patient soon became excited by the chloroform, as is usually the case, but not beyond a degree that I have often observed. Shortly after, he became more tranquil: the deceased was placed upon his side, and the operation performed, which consisted in the removal of two external tumours, and the tying of one internal tumour.
"At this moment my attention was arrested by my assistant's calling for a wet cloth: on examining the patient, I found his face and neck of a livid leaden hue or colour, the eyes turned upward, the pulse imperceptible at the wrist, and the whole body relaxed; after two or three gasps, he ceased to breathe. Every means was promptly used to restore the deceased, but without effect. The chloroform was obtained from Kent's, 91, John Street, and not exceeding three drachms was administered on a napkin. A portion of chloroform from the same phial had been administered the day before to a patient without any unfavourable effects. About ten minutes elapsed from the commencement of its administration before death took place. On making a post-mortem examination, twenty-four hours after death, I found the face less livid than before death; on examining the head, the brain and its membranes presented no other appearances than are seen in persons dying when in full health; the lungs were a good deal congested, and discharged, when cut, a large quantity of bloody serum; the heart was large, its ventricles and auricles were empty, its condition flabby, the substance of the left ventricle rather softer than natural; about half an ounce of watery fluid was found in the pericardium; the viscera of the abdomen were healthy."
This case differs from those previously related in respect to the time at which the fatal occurrence took place. It was not till ten minutes from the commencement of inhala-[137/138] tion, and when an operation which probably occupied two or three minutes had been performed, that the patient suddenly expired. The evidence of paralysis of the heart is, however, distinct enough in the absence of pulse at the wrist, and the livid hue of the countenance. In several of the previous cases, there was sudden pallor at the moment when the heart ceased to inject blood into the capillaries, but in a patient well supplied with blood, the sudden arrest of the action of the heart would cause turgescence of the veins and venous capillaries, which would be evident in the face in a few seconds. The syncope occasioned by paralysis of the heart differs from that kind of syncope which is caused by loss of blood, inasmuch as the right cavities of the heart are full in the former instance, and empty in the latter.
The circumstance of the patient having inhaled chloroform to insensibility three weeks previously, without accident or ill effects, is worthy of notice, as showing that the fatal event did not depend on any peculiarity of constitution. Although the heart was found to be empty, its flabby condition and the watery fluid in the pericardium indicate that it must have contained blood at the time of death.
Case 9 occurred on January 24th, 1849, at the Hôtel-Dieu, Lyons, where case 6 previously happened. The patient was a youth, aged seventeen, named J. Verrier, who had been employed as a miner. He was of good constitution, and was about to undergo amputation of the middle finger for necrosis of the first phalanx. The following is the account of the accident.
"As the patient's health was good, he was at once, and by his free consent, placed under the influence of chloroform. As usual, a piece of fine gauze was employed; it was spread over the face, leaving a free passage for atmospheric air; the chloroform was dropped from time to time upon that [138/139] portion of the gauze which was over the nostrils. It was administered by two assistants who were accustomed to its use, and who at the time attended to the pulse. The operator superintended the assistants. At the end of four or five minutes, the patient still felt and spoke; and at the end of another minute, he still spoke and was somewhat restless. Up to this time, from a drachm to a drachm and a half of chloroform had been employed. The pulse was regular, and of the normal strength. All at once the patient raised his body, and struggled so that the limbs escaped from the hold of the assistants, who however seized them quickly, and replaced the patient in his position. Within a quarter of a minute, one of the assistants stated that the pulse at the wrist had ceased to beat. The handkerchief was removed. The countenance was completely altered. The action of the heart had altogether ceased; the pulse could not be felt anywhere; and the sounds over the region of the heart could no longer be heard. Respiration still continued, but it became irregular, weak, and slow; and at length ceased completely in the space of about half a minute.
"The extreme danger of the patient was manifest, and immediate and energetic means were employed to rouse him. Ammonia was held to the nostrils, and rubbed in large quantity over the surface of the chest and abdomen. It was also applied to the most delicate parts of the skin, e. g., the lips and the extremity of the penis, with a view to excite irritation. Mustard was used; the head was inclined over the bed; and, finally, an attempt was made to restore respiration by means of alternate pressure on the abdomen and chest. After two or three minutes, respiration reappeared, and even acquired a certain fulness, but the pulse nowhere returned. Frictions were continued. Respiration became again slower, and at length ceased. Artificial inflation was practised, at first through the mouth, and after-[139/140] wards through the larynx, by passing a tube through the glottis, as it was perceived that air had passed from the mouth into the stomach. The precordial, epigastric, and laryngeal regions were energetically cauterised with a hot iron. The pulse did not return. For the space of half an hour every effort was made to resuscitate the patient; but in vain.
"The autopsy could not be made until seventy-two hours after death. The temperature being low, the body showed no signs of decomposition; there was still rigidity of the limbs. The features were not altered. The examination of all the organs was made with care.
"The stomach contained about one ounce and a half of a thick fluid, of the colour of the lees of wine, in no respect resembling an alimentary fluid. The organ was distended with gas, as was also the rest of the alimentary canal, which was otherwise sound. The liver and spleen were somewhat congested.
"The heart, which was normal in volume, was flaccid and empty, contained neither blood nor air. The ventricular parietes were moistened by a fine, very red foam, as if from the presence of a little blood, which had been, as it were, whipped by the fleshy columns of the heart. The venæ cavæ and the portal veins were distended by black fluid blood in great quantity. On the Eustachian valve there was a fibrinous clot, moderately firm, and weighing from sixty to seventy grains. It was the only clot met with in the cavities of the heart and great vessels. These cavities, which were carefully opened, did not contain any appreciable quantity of air.
"The lungs retracted on opening the chest. They presented both in their surface and in their substance a very black colour; otherwise their tissue was healthy. The larynx and trachea presented no lesion. The brain was [140/141] normal. The sinuses of the dura mater contained a considerable quantity of black uncoagulated blood."65
In this case every precaution appears to have been taken, except that which is the most essential, of regulating the amount of vapour in the respired air. Arrangement was made that there should be amply sufficient air for the purpose of respiration; the patient was carefully watched by three persons at least, one of whom was constantly attending to the pulse, but with no other result than to be able to announce the exact moment when it suddenly stopped. The arrest of the action of the heart in this case took place at a time when the patient was not yet rendered insensible by the chloroform, although he had been inhaling it for five minutes. We must conclude that during these five minutes the vapour he inhaled was largely diluted with air, and that he then inhaled vapour in a much less diluted form. It is not improbable that he took a deep inspiration of strong vapour, just at the moment when he struggled violently, and within a quarter of a minute of the time when his pulse suddenly ceased.
The breathing continued a little time after the heart ceased to beat, and it is therefore very probable that, if this organ had not been irrecoverably paralysed, the natural breathing would have restored its action after a short pause, that would have attracted but a momentary attention. As the spontaneous breathing of the patient did not restore the heart's action, there is no ground for surprise that the measures adopted did not succeed.
Case 10 was that of a labourer, named Samuel Bennett. It occurred on February 20th, 1849, at a dispensary in Westminster. The patient inhaled chloroform for amputation of one of the toes. Half an ounce of chloroform was [141/142] "sprinkled on a handkerchief, and held over the mouth and nose. . . . This quantity of the agent failed, however, to produce anæsthesia, having caused only the ordinary excitement and struggling." After a delay of two hours, more chloroform was procured, and half an ounce was again applied on a handkerchief, "care being taken to allow the entrance of air at short intervals." Insensibility was induced, and the toe was amputated; the chloroform being applied, as I was told, during part of the time of the operation. At the close of the operation, no blood escaped when the pressure was removed from the arteries; the patient was in fact dying, and in a short time expired. "A few inspirations were noticed after the pulse had ceased at the wrist."66
The lungs were of a dark venous hue throughout, a large quantity of blood escaping from them when cut into. Mucous membrane of trachea and bronchi congested. Heart rather large but flabby; auricles empty; each ventricle contained about an ounce of semi-fluid blood (the lungs had been inflated). Head: sinuses and veins contained blood, but not to any remarkable amount. But few bloody points occurred in cutting into the cerebral mass. Kidneys congested.
The failure of the first attempt to cause insensibility in this case, when so large a quantity of chloroform was used, illustrates very forcibly the uncertainty and irregularity of the way in which it was administered. On the first occasion only excitement and struggling were produced, and on the next the patient died suddenly.
Case 11 occurred on August 23rd, 1849, at Langres, France. The subject of it, Madame Labrune, was reported to be a healthy married woman. She inhaled chloroform with the intention of having a tooth extracted. "Complete [142/143] insensibility was not produced at the first trial: more chloroform was placed on the handkerchief, and she drew a full inspiration. Her countenance immediately became pallid; her features were visibly altered; there was dilatation of the pupils, with a convulsive rolling of the eyes; and no pulse could be felt. Every attempt was made to restore life, but without success. She died as if struck by lightning."67 The instantaneous arrest of the circulation, on a full inspiration being taken, immediately after more chloroform had been placed on the handkerchief, is particularly worthy of notice. The heart was paralysed, in this instance, as quickly as in experiment No. 25, above related.
No inspection of the body is reported in this case.
Case 12 is the first which occurred in any of the hospitals in this metropolis. The following is the account of it.
"John Shorter, aged forty-eight, a porter, known to Mr. Solly for some time as a very active messenger, habits intemperate, but apparently in perfect health, was admitted into George's ward, under Mr. Solly, on the 9th October, 1849, suffering from onychia of the left great toe, which had existed some time. It was determined to remove the nail, the man having decided before entering the hospital on taking chloroform.
"On Wednesday, October 10th, at a quarter to two P.M., he began to inhale the chloroform with one drachm in the inhaler. It had no visible effect for about two minutes; it then excited him, and the instrument was removed from the mouth, and about ten drops more were added; he then almost immediately became insensible; the chloroform was taken away, and the nail removed. He continued insensible; and, his face becoming dark, the pulse small, quick, but regular, respiration laborious, his neckerchief was removed, [143/144] and the chest exposed to fresh air from a window near to the bed; cold water was dashed in his face, the chest rubbed, and ammonia applied to the nose. After struggling for about a minute, he became still, the skin cold, pulse scarcely perceptible, and soon ceased to be felt at the wrist; respiration became slow and at intervals, but continued a few seconds after the cessation of the pulse. Immediately on the appearance of these symptoms, artificial respiration was commenced by depressing the ribs with the hands and then allowing them to rise again until the proper apparatus was brought, when respiration was kept up by means of the trachea tube and bellows, and oxygen gas introduced into the lungs by the same means. Galvanism was also applied through the heart and diaphragm, but all signs of life ceased about six or seven minutes after the commencement of inhalation. These means were persisted in until a quarter past three, but to no purpose. On removing the inhaler, the sponge, which only contains one drachm, fell upon the floor, and the chloroform splashed about,--thus showing that a considerable part of the chloroform remained unused; so that the patient could not have inhaled more than a drachm. Every endeavour was made to procure a post-mortem examination, but in vain."68
The above account is published in the Medical Gazette as communicated by Mr. Solly, but it is clearly not written by him, and it presents a very confused narrative of what occurred. If we are to understand the events in the sequence in which they are related, we must conclude that the patient became insensible and had the operation performed, that he then exhibited alarming symptoms for which cold water was dashed in his face and other measures were employed, and yet that after this he struggled for about a minute. This would be a state of things incon-[144/145] sistent, in my opinion, with death from chloroform; but possibly the proper sequence is not observed in detailing what occurred. There is some obscurity also about the amount of chloroform used in connection with what remained on removing the inhaler. If the sponge was adapted to hold a drachm in the proper manner, the chloroform could not splash about on its falling, unless there was a good deal more than a drachm in it. But whatever was the quantity of chloroform remaining in the sponge, as it was in a condition to splash about, it is difficult to perceive what prevented the liquid chloroform from dropping into the patient's throat, as he lay on his back in bed. Chloroform is as pungent as the essential oils. I have been informed of a case in which a patient was nearly suffocated by one drop falling into the throat; and the narrative of what occurred to Mr. Solly's patient is not at all inconsistent with death from spasm of the glottis arising from this cause. If, however, the patient died from the vapour of chloroform, we must conclude that he inhaled it at one moment not sufficiently diluted with air.
The chloroform in this case was administered by a non-medical person--a sort of surgery-man. After this accident, however, the chloroform in St. Thomas's Hospital was always entrusted to some one belonging to the profession.
Case 13 occurred at Shrewsbury, to a Mrs. Jones, a patient of Mr. Clement, surgeon, who had partly performed the operation of excision of the eyeball, when his patient suddenly died. Mr. Clement has, I believe, not published any account of the case, but the evidence which he gave at the inquest was reported in various local newspapers, and copied into the medical journals. The death was very characteristic of the effects of chloroform vapour not sufficiently diluted. Mr. Clement is reported to have said: [145/146]
"He gave her but a small dose to commence with, imbibed from a sponge, and then commenced the operation. Finding that did not make her insensible, about a drachm more was poured on the sponge, which she inhaled again for a few seconds. He then went on with the operation, and shortly afterwards heard a peculiar sound, which he could not describe, and she died in a moment; all the attempts to rouse her proved ineffectual. She spoke in Welsh before she died, but so quickly that he did not know what she said; he had no doubt that she died from the effects of the chloroform."69
Case 14 occurred at Berlin. The subject of it was a young lady twenty years of age, of good health, well made, and of a good constitution. The chloroform was inhaled for the extraction of a tooth. It was administered on a sponge, covered with a napkin. The dentist who administered it was not a medical man. He made five unsuccessful attempts to extract the tooth under chloroform. Three of these attempts were at nine in the morning, and two about noon, just before the accident. His patient suddenly died almost at the commencement of the last attempt to administer chloroform, stretching herself out, and frothing at the mouth at the moment of death; the countenance at the same time becoming livid.
An examination of the body took place fifty hours after death, when putrefaction had set in.
"The lungs presented nothing morbid; the bronchi contained a little bloody froth. The blood was of the colour and consistence of cherry juice. The heart was soft, flabby and collapsed. Its coronary vessels and cavities were empty, and presented the bluish-red discoloration of decomposition."70 The other organs were healthy. [146/147]
Case 15 occurred in the public hospital of Kingston, Jamaica, on January 29, 1850. The name of the patient was William Bryan, his age is not stated, nor the nature of the operation he was about to undergo. He had previously, however, undergone the operation of amputation of the penis, on account of cancer of that organ, but it was performed without chloroform. Mr. Maygarth, the surgeon who administered the chloroform, stated as follows: "I had about a drachm poured on the sponge, and applied it over his mouth and nostrils, but at first not in close contact--at no period was the atmospheric air totally excluded. He bore it badly, and I was frequently obliged to withdraw it, to facilitate his breathing. The stage of excitement which is usual came on, and he struggled and kept away the sponge for some seconds; it was again reapplied, when, after a few more seconds, observing that he made one stertorous inspiration, I removed it altogether. He ceased to breathe but after some seconds had elapsed, made another inspiration, and this occurred several times, until at length respiration ceased entirely." The measures which were employed were of the usual kind, but were of no avail.
The brain and its membranes were found to be congested. The lungs were congested, especially posteriorly. The right side of the heart contained dark fluid blood, and the inner surface of its left cavities, and of the aorta, were stained with blood. There was some disease of the aortic valves, and the heart had undergone some amount of fatty degeneration.71
Case 16. In February 1850, a death from chloroform occurred on board ship at the Mauritius. A report of the case was sent to the Board of Ordnance, and also to the Admiralty. The secretary of Sir William Burnett first in-[147/148]formed me of the case, and a day or two afterwards I had an opportunity, through the kindness of the late Marquis of Anglesey, of reading the report which was sent to him as Master of the Ordnance, and I made a note of the chief particulars as soon as I got home. As the report was a very able one, it is to be regretted it has not been published. The accident occurred to an artilleryman, aged 24, who required to have the last phalanx of the middle finger removed. In other respects, he was considered to be in good health. Two scruples of chloroform were first poured on the handkerchief with which it was administered, and then one scruple more. It was observed that the face turned pale, and the pulse and breathing ceased, soon after the chloroform was discontinued. The measures which were employed to restore him were of no service. The lungs after death were found to be emphysematous; and, upon inquiry, it was ascertained that he had been short of breath on exertion. The right cavities of the heart were filled with fluid blood. The sinuses of the dura mater contained less blood than usual, and the brain was pale. The medical man reporting the case considered that the emphysema was the cause of death, by interfering with expiration, and thus detaining the vapour; and it must be admitted that, if the vapour were not sufficiently diluted with air, the emphysema might increase the danger. I have, however, administered chloroform in several cases in which emphysema existed to an extreme degree, without any ill effects; consequently, when the vapour is properly diluted with air, this affection appears to be no source of danger.
Case 17 was that of a patient of Professor Carl Santesson, in the Seraphim Hospital at Stockholm. I was indebted to Mr. Paget for my first information about this case, and to Dr. W. D. Moore, of Dublin, for some further particulars respecting it. [148/149]
The patient, a man thirty years of age, was affected with hydrocele, and there was some suspicion of disease of the testicle. It was consequently intended to operate on the hydrocele by incision, in order that the testicle, if diseased, might be removed. The chloroform was administered in the same way that Professor Santesson had seen it exhibited by Dr. Simpson, except that it was poured on a little cotton, which was placed at the small end of the cone, into which the folded towel he made use of was rolled. About a drachm and a half was first poured on the cotton, and the patient was told to inhale in long and deep inspirations. This quantity being nearly evaporated in two or three minutes, a drachm more was added. After a few inspirations rigidity and struggling came on: these subsided, but in a little time returned more strongly than before, and the towel was removed from the face until the struggling ceased. The patient, however, not being sufficiently insensible to undergo the operation with the necessary quietness, the towel was reapplied, when, after a few inspirations, the pulse suddenly ceased. The face and the whole surface of the body turned pale, the eyes rolled upwards and inwards, and the breathing became very slow, but full and deep, the intervals between the inspirations becoming longer, until the respiration ceased altogether. The patient died before the operation was begun, and within five minutes from the commencement of inhalation. During the application of various means of resuscitation, including the dropping of cold water guttatim on the epigastrium, the breathing returned, and continued for the space of three or four minutes; but the pulse and sounds of the heart did not return.
At the examination, thirty-two hours after death, the dura mater was found to be congested, and there was considerable serous effusion between the membranes of [149/150] the brain. There were also some bony deposits under the dura mater, and some adhesions of the arachnoid, indicating long standing disease of the membranes.
The heart was of normal size, and flaccid; the vessels on its surface strongly distended with blood. The left ventricle was empty; the left auricle, on the contrary, and the entire of the right side of the heart, with the great veins, were filled with thin uncoagulated blood. In the right ventricle only was a little loose coagulum found. The lungs, posteriorly, were highly congested, exhibiting here and there infiltrations of blood from the size of a pea to that of a small hazel-nut. The pulmonary tissue was otherwise sound; giving, however, when cut into, the odour of chloroform, but more feebly than the brain did. The mucous membrane of the larynx and bronchial tubes were slightly reddened from sanguineous congestion. The blood was everywhere of the same thin juice-like nature.72
Case 18. I am indebted for my information respecting this case to Dr. James Adams, of Glasgow, who was good enough to send me a copy of the notes respecting it, from the case book of his colleague, Mr. Lyon, in whose practice, in the Glasgow Infirmary, the case occurred, in March 1850. The patient was a boy seven or eight years old, from the Highlands, whose health was considerably impaired by years of suffering from calculus. Mr. Lyon says, "being laid in bed, I placed a piece of lint, moistened with chloroform, near to his face, when, in a few minutes, he ceased crying. I now told my clerk to take charge of the chloroform, and introduced the sound. I thought I detected a calculus, but could not hear the click distinctly, in consequence of the patient moaning. One of the bystanders held his hand between my ears and the patient's face, when the click was [150/151] at once heard. I withdrew the instrument, and was horrorstruck with the livid countenance and vacant eye of the patient; the cardiac and radial pulses were gone, and, making one deep gasp, he was to all appearance dead." Artificial respiration and other measures were employed without effect. "The external jugulars being remarkably turgid, and the face still very livid, the right jugular was opened, when several ounces of dark blood flowed rapidly." This measure, and galvanism, which was applied afterwards, were of no avail.
Case 19. The subject of this case was Alexander Scott, aged thirty-four, a police constable, who died in Guy's Hospital in June 1850, whilst undergoing an operation for the removal of a portion of the right hand. Mr. Cock, the operator, said that he was certain there was no disease about the patient. He described the accident as follows:--"The ordinary machine was used, and, as it had not the effect, witness directed that a napkin should be folded into the shape of a cone, which was applied with chloroform. The occupation of removing a portion of the bone occupied one minute and a half, but before it was completed, the blood which was gushing out, suddenly stopped, when witness directed Mr. Lacy to feel the pulse of deceased, and they found that deceased had expired."73
The sudden stopping of the hæmorrhage shews that, in this case, as in the others, the action of the heart was suddenly arrested. The first attempt to cause insensibility failed in this as in some other cases.
Mr. Cock tried to dissuade his patient from having chloroform, severe as the operation would have been without it. In Guy's Hospital and St. Thomas's the medical officers had a strong objection to narcotism by inhalation [151/152] for the first two or three years after the practice was introduced, and chloroform was used much less generally in these institutions than in any other of the hospitals of London; yet it was precisely in these two hospitals that two deaths from chloroform occurred, before any such accident had happened in any other hospital in this metropolis. This circumstance is worthy of the consideration of those who propose to limit the accidents from chloroform by restricting its use to a few great operations.
In this case the lungs were reported to be extremely congested. Heart flabby, not particularly distended; about two ounces of fluid blood on the right side; not more than half an ounce on the left. Head.--Much congestion of the dura mater; the grey matter of the brain was dark and congested; fluid was found in the subarachnoid space; and a considerable quantity of it in both ventricles. Kidneys congested.74
Case 20 occurred on September 20th, 1850, at the Cavan Infirmary, Ireland. The case occurred in the practice of Dr. Roe, and I am indebted to Dr. Robert Adams, of Dublin, for a manuscript account of it. The name of the patient was James Jones, and his age twenty-four years. Chloroform was exhibited with the intention of performing amputation below the knee, on account of scrofulous disease of the ankle, with ulceration of the cartilages. The patient was reduced to a state of great debility by the disease, and was suffering from hectic fever, but had no cough. The following is Dr. Roe's account of the accident:--
"When placed on the operating table the heart's action was very quick and weak, but he did not appear more faint or pale than usual. I then saw Mr. Nalty, the apothecary, measure one drachm of the chloroform in the small minim [152/153] glass measure, and pour it upon a little folded lint, which was placed in an oval hollow sponge, held in the hand with a small towel. Recollecting I had used this chloroform in another case, and finding some delay in producing the anæsthetic effects, I directed Mr. Nalty to add thirty drops more to that already put on the lint. I then applied the sponge to the patient's nose, directing him to keep his mouth shut, and gave the towel into the care of Dr. Halpin, who was on the opposite side of the table, while I went to prepare myself for the operation. Mr. Bird had scarcely screwed up the tourniquette, which had been previously placed on the thigh, while I was examining the state of the circulation in the tibial arteries, and which could not have occupied one minute,--certainly the patient could not have taken fifteen inspirations,--when Dr. Halpin told me the anæsthetic effects were produced. This struck me as being unusually quick and sudden, and on removing the towel from the face, we saw a slight convulsive action of the left eyelid (the eyelids were partially open), and a small quantity of frothy saliva at the mouth. I felt rather uneasy, but not much alarmed, as Dr. Halpin said he had often seen such symptoms from the effects of chloroform, although I bad not met with them. On a more minute examination of the heart, the eyes, muscles of the limbs, etc. we found him dead."
Energetic means were used with a view to restore the patient, but without effect. No inspection of the body took place.
Case 21. The next case of recorded death from chloroform occurred in the Stepney Workhouse. The patient, named John Holden, age not stated, was about to undergo an operation on the penis. It was stated at the inquest that half a drachm of chloroform was administered without [153/154] effect, and then half a drachm more was applied, when the patient suddenly expired. This death occurred in April 1851.
Case 22 is important, as having given rise to a prosecution. The medical man, an officier de santé, named Kobelt, was accused of homicide, by imprudence, want of precautions, etc. The chloroform was administered on a handkerchief, and the accident occurred as suddenly as any of the others. The husband of the patient stated that the whole process did not last a minute. "I observed attentively," he said, "during this time, and the character that her countenance took all at once made me apprehensive. I spoke of it to the operator, who tranquilized me, and continued to extract the teeth. After the third tooth, however, he partook of my apprehension, suspended the operation, and proceeded to adopt measures indicated by the circumstances." Professor Sédillot, who had to pronounce an opinion on the case, after hearing all the evidence, said, "I do not think that M. Kobelt is guilty of imprudence or of rashness, because that officier de santé has followed a practice very habitually employed, and even recommended, by eminent practitioners, whose example and authority were sufficient to inspire him with security, and shade him from reproach." The accused practitioner was acquitted. The above remark of Sédillot applied to the plan of causing insensibility very rapidly, as first recommended by Dr. Simpson and he added some observations, to the effect that, when used in a different manner, chloroform is free from danger.
The above case occurred at Strasbourg, on June 10th, 1851. The name of the patient was Madame Simon, and her age thirty-six. After death the lungs were found to be somewhat congested, and emphysematous. Heart flaccid, of [154/155] middle size; right cavities filled with liquid dark-coloured blood, mixed with some fibrinous clots. The left cavities contained similar blood in much smaller quantity.75
Case 23 occurred on July 8th, 1851, at the Seaman's Hospital, Greenwich. The patient was a light-coloured mulatto, aged forty-five, native of New York. He died during the operation of removing the left testicle, which was disorganized by suppuration. "The chest had been carefully examined a few days previously, both by percussion and auscultation. No physical signs of disease were detected. His pulse was regular and feeble, about seventy. He was rather nervous, and fearful of the operation. No arcus senilis. After taking a glass of wine he commenced the inhalation, twenty minims of chloroform having been poured on a linen cloth. At the expiration of a few minutes, this had been dissipated, producing only very trifling excitement; a second dose, of the same quantity, was then administered in the same way; the man began to sing and shout, his expressions relating to the firing of guns. The second quantity having been exhausted, and the effects of the chloroform becoming more apparent, but sensibility being still perfect, and even intelligence almost unaffected, a third quantity, of ten minims, was poured out, and, afterwards, twenty minims more. Having passed through the usual convulsive stage, and insensibility being established, the further administration of chloroform was desisted from at the end of about seven minutes, though this time is merely guessed at; it might have been more, but was certainly not less. At this time the respiration was unembarrassed, and the pulse regular, and about seventy, with as much volume as before the inhalation. The lips were florid; in fact, the chloroform appeared to have acted [155/156] in the most benign way. Mr. Busk commenced the operation by an incision through the scrotum, which divided a small arterial branch, and some enlarged veins, from which the blood flowed pretty freely. The flow, however, almost instantaneously ceased, and Dr. Rooke, who kept his finger on the man's pulse, found that cease at the same moment. Respiration appeared to cease almost instantaneously with the heart's action. Regular respiration at least did; for, while we were looking at the man's face, he fetched one or two sigh-like inspirations. The ribs and abdomen were compressed, so as to induce inspiration and expiration; the lungs were inflated by blowing through the nostrils, the larynx being compressed against the spine, and, for three or four minutes, upon our efforts being suspended, the man occasionally took an inspiration; on one occasion three or four in succession, so as to make us flatter ourselves that he would come round. . . . It is worthy of remark that, for a long time after spontaneous respiration had ceased, the lips retained a florid colour. The muscles were all relaxed, and the veins on the side of the neck turgid."76
At the inspection of the body next day, the vessels of the dura mater, and those on the surface of the brain, were gorged with fluid blood. The lateral sinuses also afforded a flow of dark-coloured blood. There was a considerable quantity of serous fluid in the cavity of the arachnoid and in the spinal sheath. The substance of the brain was very soft. (The weather was warm.) The lungs were of a dark purple colour posteriorly, and much loaded with fluid blood and serum, but were everywhere crepitant and healthy. The external surface of the heart was covered almost entirely with fat; in some parts to a considerable thickness. There were two fibrinous spots on its surface. No fluid in [156/157] the pericardium. The venæ cavæ were full of fluid blood. On removing the heart, a white fibrous coagulum, about as big as a walnut, was found in the commencement of the pulmonary artery. The heart was uncontracted, and the cavities contained a very small quantity of dark fluid blood. The walls of the right ventricle, and of the left auricle, were thinner than natural. Some portions of the substance of the heart were paler than natural:--"In these paler portions of the muscular substance, the fibres had, for the most part, lost their striated aspect, and had become converted into a fine granular material contained in the sarcolemma. Here and there a minute oil-globule could be observed in the muscular fibrillæ, but nowhere did this amount to fatty degeneration."
In this case all the precautions appear to have been taken which are possible in making a patient insensible with undiluted chloroform, administered on a handkerchief and the case, therefore, strongly confirms the proposition that chloroform cannot be administered in this way with perfect safety.
The patient was apparently in the most satisfactory condition at the conclusion of the inhalation, and yet, a few seconds afterwards, the heart suddenly ceased to beat, from the effect, as we must conclude, of that portion of vapour which was in the lungs at the moment when the inhalation was discontinued.
Case 24 occurred in October, 1851, at Chipping Norton, Somerset, to a patient of Mr. Farwell, named Elizabeth Hollis, and aged 37. No one observed the manner in which the breathing and circulation ceased, and, as the patient was in a state of extreme debility, it is not quite certain that the chloroform was the sole cause of death. It was administered to prevent the pain of removing the fæces, which [157/158] became impacted in the rectum on account of extensive cancerous disease of the uterus and vagina. The surgeon reports that "the time occupied in the inhalation was about eight or nine minutes; quantity inhaled 10½ drachms, half a drachm at a time, allowing her frequently to breathe the atmospheric air. She spoke to me during this period. When I found that her arm fell after being raised, I proceeded to and accomplished the operation. At this time she was not inhaling. I then, as I always do, wetted the face with a sponge, with the view of washing off any remaining chloroform from the nose and lips, when, to my surprise, I found that she had ceased to breathe, and all attempts to restore her were in vain. . . . When I commenced the operation, the pupil was contracted, and the conjunctiva slightly red. After death, the pupil was very dilated, and the countenance extremely pallid."77 There was no inspection of the body. This patient had inhaled chloroform on two previous occasions for a similar operation.
Case 25 occurred in St. Bartholomew's Hospital, on March 17, 1852. Thomas Hayward, aged 23, was suffering from aneurism by anastomosis, occupying the right ear and its neighbourhood. He had inhaled chloroform on the 14th of the previous month, whilst Mr. Lloyd placed ligatures on the temporal artery and some other arteries supplying the tumour; and it was with a view to tie an additional artery, situated between the mastoid process and the ramus of the jaw, that chloroform was again administered.
"The chloroform was some of the same, and the apparatus employed for its administration precisely similar (alluding to the former occasion.) It was administered by one of Mr. Lloyd's dressers, who well understood, and had great experience in its use. A gentleman of great experience, who [158/159] had been for years at the hospital, and two years house-surgeon, was watching its effects, and marking the state of the pulse. Other gentlemen were assisting, and also on the look out.
"In from five to ten minutes the usual effect was produced, the patient having previously struggled much. The operation was then commenced; but no sooner had Mr. Lloyd cut the skin, than it was stated that the pulse had suddenly ceased. The chloroform was at once removed; but in a few seconds, the patient had ceased to breathe, and no pulsation could be felt at any of the arteries or the heart.
"Artificial respiration, as well as percussion and compression of the different parts of the body, were immediately employed with energy; and, after continuing the means for a short time, the circulation was observed to be returning, and the act of respiration was several times performed. The state of inanimation, however, speedily returned; but, by the employment of the same means as before, with the use also of galvanism, the circulation and respiration were again restored. Quickly, however, the patient fell into the same state as at first, but was again restored by the same means.
"In a few minutes the state of inanimation again returned, when the external jugular vein, which on the right side was very turgid, was opened, and tracheotomy was performed, and the lungs inflated. The patient was also placed in a warm bath, at the temperature of 104?, artificial respiration being kept up all the time. All, however, was of no avail."78
At the examination of the body, the following are amongst the appearances noted. "The venæ innominatæ and vena cava superior were full of blood, and probably would have been distended, but that two or three ounces of blood had flowed into the coffin from the opening made into [159/160] the external jugular vein. The right auricle and ventricle were distended with blood, and would probably have been more so but for the escape of blood mentioned above. The left auricle and ventricle contained very little blood; the left ventricle was perfectly contracted in the rigor mortis. The heart was of full size. It appeared in every part natural in its texture, and as if it had possessed full power. Its valves also were all healthy; neither could any disease be found in any of the chief bloodvessels within the chest. All the blood, however, was fluid, and it remained without coagulation after its escape from the heart and vessels. It had also a brownish purple hue, much like that which is commonly observed in the spleen: none of it, when thinly spread out, presented the ordinary dark, black, or crimson hue of venous blood. Both lungs were attached by old adhesions about their apices and posterior surfaces, but these were of small extent. Their texture was healthy, but they appeared more than usually collapsed and dry. Their blood-vessels were not over filled."79
In this case, every precaution seems to have been taken, except that one which is most essential of all, of regulating the proportion of vapour in the inspired air. It had always been made a great point in St. Bartholomew's Hospital to attend to the pulse very carefully,80 and on this occasion it was closely examined, but only, as in some other cases, with the result of being able to note the moment when it suddenly ceased.
With regard to the return of the circulation, which is mentioned in the report as having occurred on three occasions, together with the breathing, during the efforts at resuscitation, I understood from inquiries I made of a gentleman present, that this was judged of from the red [160/161] colour returning to the face and lips, but that the pulse and sounds of the heart were never distinctly perceived after they first ceased. The respiration may cause the colour to return to the face without a true circulation, as I have seen whilst inflating the lungs of still-born children; for if a portion of red blood be mechanically displaced from the lungs by the motion of the chest, it will be propelled by the contractility of the arteries, which continues for some time after death.
Case 26 is related by Dr. Majer, of Ulm.81 It occurred on June 27th, 1852. The patient, Madame W., was 32 years of age, and of good constitution. She was in very good spirits, and was only waiting the operation of having a tooth extracted, before going to dinner. It was stated that only twenty or twenty-five drops of chloroform were put on a sponge, which was surrounded by a handkerchief. After four or five inspirations, the operator inquired if his patient did not feel a singing in the ears. She replied with a trembling and thick voice. At the same time she stretched out her limbs, the face became bluish, the eyes haggard, the head and the arms fell--she was dead. The patient's husband said, that the time between the inhalation and death was so short that one could scarcely have said Yes or No.
An examination of the body was made twenty-five hours after death. Putrefaction had commenced, and the body was not rigid. The vessels of the membranes of the brain were gorged with blood containing many bubbles of air. The heart was soft and flaccid; the coronary vessels were engorged with blood and air; the cavities of the heart contained air, but little blood. The lungs were congested at the inferior parts. [161/162]
Case 27 took place at Melbourne, Australia. The name of the patient was Mr. John Atkinson, but his age is not stated. Dr. Thomas, who was about to operate for fistula in ano, said: "Before administering the chloroform, I asked the deceased particularly if he had ever suffered from any serious illness, to which he replied in the negative. I also inquired whether he had been subject to cough or palpitation, and he answered that, some time ago, he had suffered slightly from cough. The pulse was good, and Mr. Barker proceeded in the usual manner to administer the chloroform, which shortly produced convulsive twitchings of the muscles. I then went to the door to request the nurse to send up some person to assist in holding the patient in a proper position for the operation, and I returned to the bed, and poured a little more chloroform on the handkerchief; when it was applied to the face, I heard him splutter at the mouth; the chloroform was instantly discontinued, but the patient suddenly expired. We tried all the means usually resorted to in other cases of suspended animation, but without effect. I had frequently used the same chloroform in other cases. It was not more than a minute after the first application of chloroform that death occurred. About a drachm had been poured on the handkerchief."
At the examination after death, "there was considerable serous effusion into the pericardium, and the heart itself was larger and more flabby than usual. It was hypertrophied, and there was dilatation of the cavities; the lungs were healthy, and there was a slight appearance of disease about the liver, such as is observed in persons addicted to intemperance."82
Case 28. On August 10th, 1852, a Mr. Martin, a cattle [162/163] dealer died near Melrose, in Scotland, after inhaling chloroform for the application of potassa fusa to some ulcers of the leg. Dr. W. M. Brown, who relates the case, says:--"Before proceeding to apply the caustic I gave him chloroform. He was not easily affected by it, and struggled a good deal. After beginning to apply the caustic I found he was not sufficiently insensible to pain, and gave him a little more chloroform, which had the desired effect. I then proceeded with the application of the caustic, and was just finishing, when I observed a sort of catch in his breathing. I immediately stopped, and, on looking at him, I saw the mouth and eyes open, the breathing irregular, the face pale, the eyes slightly turned upwards, and the pupils dilated." Dr. Brown tried artificial respiration and other means to resuscitate the patient, but without effect. He says, "in a few minutes the man died." The pulse is not mentioned, nor the age of the patient.83
Case 29 took place in the Manchester Royal Infirmary, on December 24th, 1852, during the removal of a malignant tumour of the thigh, by Mr. Jordan. The patient was Henry Hollingsworth, a factory operative. His age is not stated. "The man was very much excited, struggled and talked fast. The chloroform was administered slowly, and every precaution was taken to prevent any danger, and the medical men remarked two or three times how very long it was in taking effect. He at last became insensible, in about seven minutes at least. Mr. Jordan commenced the operation by an incision into the skin covering the tumour[.] I was assisting the surgeon when Mr. Heath directed my attention to the patient's face. This was about five minutes after the operation had commenced. I then observed congestion about the face, but there was no stertorous breath-[163/164]ing. His pupils appeared almost to have ceased to act. His breathing was becoming exceedingly slow, and he seemed to be sinking fast. I directed the attention of the operator and the other medical men to these symptoms. The operation was then suspended, and means were resorted to for restoring animation, but the pupils had ceased to act, and had become fixed almost immediately. He gave one strong gasp, and then to all appearance was dead. In administering the chloroform, successive doses were given until it took effect. Every dose consisted of a drachm, taken, at intervals, in an inhaler."84
The following remark is made respecting the autopsy. "The post-mortem examination shewed that asphyxia, caused by chloroform, produced the death. There was a congestion both of the brain and lungs." The appearances met with after death from chloroform do not indicate the way in which death has taken place. In animals that are killed by it, the right cavities of the heart are always found filled with blood, whether they die suddenly by its direct action on the heart, or more slowly by its effects on the brain, and the breathing ceases before the circulation. The lungs are seldom much congested in animals, whichever be the mode of dying, and the appearances in the head are not unusual. The state of the pulse is not mentioned in the above account of the case; but congestion about the face was first observed, and then it was noticed that the breathing was getting slow. It is sufficiently probable that the breathing ceased on account of the action of the heart being first arrested; but even if the respiration was embarrassed by the action of the chloroform on the brain, it is pretty certain that that agent also acted directly on the heart; for it cannot be supposed that the means used for restoring animation would have failed, if the heart had been acting properly when the breathing ceased. [164/165]
Case 30 took place on March 19th, 1853, in University College Hospital, London. The subject of it was an un-married woman, named Caroline Baker, aged twenty-eight. The chloroform was administered with the intention of applying nitric acid to a sloughing ulceration of the labia and vagina. "The chloroform, supposed in the first instance to be about a drachm, was poured on lint about five inches square, and folded four or five times over. After a short time the patient became restless, talked loudly, and threw about her arms. Soon afterwards a partial relaxation of the limbs took place, and she became insensible and pulseless."85
Further symptoms are not given, but it is stated that she sank and died. The breathing is not mentioned, but Mr. Erichsen, who, although not present at the accident to his patient, would be made aware of all that occurred, stated at the inquest, that death was produced by a paralysis of the heart from the influence of the chloroform. Dr. Quain examined the structure of the heart with the microscope, and he "found that organ, particularly on the right side, in a state of fatty degeneration."
Case 31 was communicated to the Society of Surgery of Paris by M. De Vallet, Surgeon-in-chief to the Hôtel-Dieu, d'Orléans. "A soldier of the line, aged twenty-five, apparently in good health, and of strong frame, consulted M. Vallet for a small tumour situated behind the right labial commissure. Before operating, he proceeded to direct the inhalation of chloroform. The patient, fasting, being placed in the horizontal posture, the chloroform (about one gramme) was poured upon a hollow sponge, and applied to the nose, the mouth being left free. At the expiration of a minute, no effect having been produced, four grammes [165/166] were poured on the sponge, and at the expiration of four minutes, the patient, without having experienced any irritation of the larynx, without having manifested any resistance, without redness of the countenance, and after only a slight period of agitation, fell into a state of insensibility fit for the operation. Scarcely had the incision been made, necessary to expose the cyst, when the patient became pale, respiration was suspended, and he sank into a state of complete collapse. All the usual remedies were tried, and without avail. M. Vallet opened the trachea, and performed artificial respiration with an elastic tube; then an electric current was sent by needles through the region of the heart. The patient died without any sign of reaction.
"Examination of the body.--The vessels of the brain were empty; the lungs were congested with blood, which in some situations was extravasated; the heart was excessively flaccid; there were some soft clots in the right cavities; the left were empty. The stomach was full of gas; the liver, spleen, and kidneys were gorged with black blood."86
Case 32 occurred in the Royal Infirmary of Edinburgh to a man aged forty-three, on whom Dr. Dunsmure was about to operate for stricture of the urethra by perineal section. The chloroform was administered by Dr. Struthers. About an ounce of chloroform was used, and the patient had been put under the influence of this agent on two former occasions, when a similar quantity was employed without ill effect. The following is Dr. Dunsmure's account of the case:--
"While the patient was inhaling the drug, he struggled considerably, and became a good deal congested in the face and head. He seemed to take a slight convulsion, like an epileptic fit, and such as I have seen on several occasions [166/167] in people who have led an intemperate life. During the convulsion, the handkerchief containing the chloroform was removed to some distance from the face. In a short time the inhalation took effect, and he began to snore, and although still violent, the chloroform was removed from the face entirely, and the handkerchief placed under the pillow. As soon as the patient became more quiet, he was pulled down on the table, and placed in the proper position for the operation. I then shaved the perineum, and was just going to make my first incision, when one of the assistants said that his pulse was becoming weak. The posterior tibial, Mr. Spence then remarked, was good, but in a second or two after, both gentlemen exclaimed that the pulse was gone. I rushed from my seat to the patient's head, and found that his breathing had ceased. Those present who had an opportunity of observing the respiration, which I had not, owing to the stool on which I sat being low, positively assert that the breathing did not cease before the pulse. The face was much congested, the jaws were firmly closed, and the pupils were dilated. I immediately forced open the lower jaw by means of the handle of a staff, and with catch forceps pulled out the tongue. Artificial respiration was had recourse to, and in a few minutes he made a long inspiration. This was soon followed by a second, by a third at a longer interval, by a fourth at a still longer period, and then by a fifth, when all attempts at natural breathing ceased. No pulsation could be felt in the radial arteries. The chest was noticed to be much contracted, to have apparently lost its elasticity, and not to expand when the ribs were forcibly compressed during the artificial respiration. I had previously sent for a galvanic apparatus, which was in the flat below, and it arrived almost immediately after the patient had made the fifth inspiration. When the tongue was pulled out, and before [167/168] the first breath was taken, I was on the point of opening the trachea, but this proceeding was then abandoned; it was now, however, had recourse to, in order to carry on artificial respiration more certainly: the external jugular was also opened, and about a couple of ounces of blood flowed. By the time the tracheotomy tube was inserted, the galvanic apparatus was in working condition, and it was applied on each side of the diaphragm. It acted remarkably well; at each application of the sponges, the muscle descended as if the patient was in life; air passed through the tube in the trachea, and for some time I was in great hopes that the man was to be saved; but the muscle gradually lost its contractility, and although the galvanism was kept up for an hour, it was evident that all our efforts were in vain--that life was extinct. The post-mortem examination was made the following day at one o'clock, rather more than twenty-four hours after the patient's death, and I give the report of it as drawn up by Dr. Gairdner, the pathologist to the Infirmary:--
"John Mitchell, aged forty-three, died 28th September. A very robust man; height five feet eight inches; diameter (lateral) of base of thorax, ten and a half inches.
"External appearances.--Considerable lividity of face and neck, and more than usual congestion of depending parts. Considerable amount of fat, but more in omentum and around viscera of abdomen than in external parietes.
"Chest.--Right pleura presents a few slight adhesions near the middle; left pleura free. No fluid in either pleural cavity. Pericardium contained about half an ounce of serum, and presented a few opaque patches on its surface. Both sides of heart contained blood, the right side rather more than the left. Blood more than usually fluid. External fat of heart considerable, about three lines on some parts of right ventricle. Muscular tissue of heart [168/169] generally flabby, and rather pale, but not distinctly disorganized to the naked eye. Valves perfectly healthy. Aorta presented very faint traces of atheroma. A few traces of atrophy of right lung towards its apex and anterior edge, but very limited. In all other respects lungs free from disease, but somewhat congested.
"Spleen soft, but not diffluent.
"Liver congested, but otherwise normal.
"Kidneys congested, but otherwise healthy.
"Brain.--The subarachnoid fluid presents considerable milky opacity, and is of moderate quantity. Moderate congestion of the meninges generally. About half an ounce of fluid in the ventricles. Substance of brain healthy. Arteries at base perfectly free from atheroma. Air passages.--Glottis perfectly patent. Mucous membrane of larynx and trachea slightly congested.
"Microscopic examination shewed the fibres of the heart to be nearly normal, though scarcely so distinctly striated as in some cases. The minute vessels of the brain and pia mater presented at some points a few clustering granules, but to no great extent."87
Dr. Dunsmure expressed the opinion that four or five minutes elapsed from the time the chloroform was left off before the pulse failed. But it is pretty certain that he has much over-estimated the time. Indeed, if the shaving of the perineum were likely to occupy even half of this time, the operator would have done it, or had it done, before the chloroform was administered. Dr. Dunsmure makes the following remark in his comments on the case: "In several instances where I have seen chloroform very nearly prove fatal, the respiration became gradually restored after an inspiration had once been made; in this case, however, no such fortunate occurrence took place." In the other cases [169/170] to which allusion is here made, the heart has not been paralysed, or at least not completely, but they show that the method of administering chloroform in Edinburgh had been far from satisfactory in its results, although no patient had before that time been actually lost.88
Case 33 occurred in University College Hospital, London, and the following account of it was given by Dr. Hillier:
"E. R., aged 40, a woman of moderate height, rather thin. The general health has been pretty good; she had not been liable to palpitation or dyspnœa. Had been in the habit of drinking pretty freely. Admitted on October 5th, at 11 p.m. She was suffering from the symptoms of strangulated hernia, which had existed two days and a half. Efforts were made to reduce the hernia, both without and with a warm bath, in which she was for upwards of half an hour without getting very faint. These efforts being unsuccessful, an operation was at once determined on. Her pulse was at this time regular, and of tolerable strength.
"Chloroform was administered in the usual way, on a piece of lint, which was held three or four inches from the patient's face, and then brought to within an inch and a half of her nose and mouth, leaving space around for the admission of air.
"For three or four minutes nothing unusual presented itself; the pulse and respiration proceeded normally. There was put on the lint, at first, one fluid drachm of chloroform; and, at the end of three or four minutes, forty minims more were added. This was the whole quantity of chloroform employed. Within a minute after the second quantity of chloroform was added, the patient struggled violently both with her arms and legs. During these struggles I was [170/171] holding her right hand, and was unable to feel the pulse in consequence of her constant motions. The struggling lasted about a minute, and on its ceasing, the patient commenced to breathe with loud, rough stertor. I at once removed the lint from before the face, and felt for the pulse, which I could not find. Immediately cold water was dashed on her face. She breathed with this stertor for two or three short inspirations, and then two or three long ones, and then the breathing ceased. Immediately artificial respiration was resorted to, and within a minute galvanism was applied to the back of her neck and the diaphragm. Under the influence of these agencies, the patient gasped about three times at intervals; after this, no further signs of life were exhibited.
"At the time when the stertor commenced and the pulse failed, the pupils were dilated, and the face of the patient was only slightly altered. The tongue was not retracted, for one of the bystanders at once put his fingers into her mouth to ascertain this."
At the autopsy made by Dr. Garrod thirteen hours after death, the rigor mortis was well marked; the blood was very fluid in all parts of the body. There was about an ounce of colourless fluid in the pericardium. The heart was quite collapsed and empty, but, as Dr. Garrod observes, this may have been due to the fluidity of the blood. The weight of the heart was seven ounces and three quarters; valves healthy. Walls of the right ventricle flabby and pale; mean thickness one eighth of an inch. At some parts the muscular substance was in a very thin layer, being much encroached on by fat. In several places there was scarcely any muscular fibre-visible. This was chiefly the case near the apex. Examined by the microscope, much fatty degeneration of the muscular fibres of the right ventricle generally was discovered. The walls of the left ventricle were flabby, dry in appearance, pale, [171/172] and very friable. Both lungs were crepitant throughout, not much engorged. Brain not congested. The intestines above the strangulation were much distended with flatus, and inflamed.89
Case 34 occurred on October 20th, 1853, a few days after the last. The patient was a young woman named Ann Smith, aged 22 years, under the care of Mr. Paget in St. Bartholomew's Hospital, who was about to apply the actual cautery to a sore of cancroid nature in the vagina. She was a stout, florid young woman, formerly of dissolute habits, but apparently in perfect health, with the exception of the local ailment. She had been put under the full and prolonged influence of chloroform a fortnight previously for the application of the cautery, without the occurrence of any untoward symptoms whatever. The chloroform was administered by Dr. Black, one of the assistant physicians.
"The usual form of inhaler was employed,--a padded metal cup, fitting over the nose and mouth, and supplied with valves. A drachm, by measure, was first poured on the sponge, but as the administration did not immediately commence, a considerable part of this was no doubt wasted; after a short inhalation, a second drachm was supplied, and subsequently the further quantity of half a drachm. The patient had gone through the usual stages of excitement, etc., and the last dose was scarcely used, as she sank off, almost immediately after its application, into a state of complete insensibility, unattended by any alarming symptoms. About five minutes had been occupied by the inhalation, and probably not more than a drachm and a half of the fluid really inhaled. The apparatus was now removed from the face, and the patient having been drawn into the proper position, Mr. Paget was about to commence the [172/173] operation, when Dr. Black, who throughout had kept his finger on the pulse, noticed it to have become extremely weak and fluttering. Almost immediately afterwards, the patient's countenance was observed to be dusky, turgid, and congested, and the respiratory movements began to be performed at long intervals, and by slight catching efforts. No time was lost; cold water was at once dashed on the thighs, face, and breast; and, the failure of the respiration becoming shortly complete, Mr. Paget immediately began artificial insufflation of the lungs, by alternately blowing into the nostrils, and compressing the chest. Just before commencing this process, Mr. Paget had ascertained, by drawing the tongue forwards and examining the glottis with the finger, that the epiglottis was not pressed down."
Other means were employed, but no further signs of life appeared. It is further recorded that, "immediately after the first alarming symptoms, the pupils were of the medium size, neither contracted nor dilated. All efforts at respiration ceased about two minutes after the first indications of failure; the pulse, however, as a very feeble flutter, was felt occasionally for at least two minutes later."90
At the autopsy, performed by Mr. Paget, twenty-two hours after death, "the thorax was first examined, and nothing whatever abnormal could be detected in any of the viscera; the lungs were healthy and crepitant in every part; their posterior lobes were not more congested than is seen in almost every examination; the heart, collapsed, but not contracted, and containing a small quantity of fluid blood in each cavity, was of normal size and proportions, in every respect, and its muscular structure, examined by the microscope, showed no degeneration. The brain, its sinuses, ventricles, etc., were all carefully examined, and neither in texture nor quantity of blood was anything abnormal detected."91 [173/174]
Although the failure of the pulse was the first symptom of danger in this case, it continued to be felt as a very feeble flutter for about four minutes, so that the heart was not so completely paralysed as in most of the fatal cases. It must, however, have been so far paralysed as to be past recovery.
Case 35. Professor Dumreicher related a case of death from chloroform at the meeting of the Vienna Society of Physicians, held on November 16, 1853. The patient was a young man, aged nineteen, in somewhat feeble health, who inhaled chloroform in the recumbent position, in order to have his anchylosed knee-joint forcibly extended. It was inhaled from a vessel resembling a snuff-box, which was held to the nostrils. "The inhalation was continued for fifty seconds, and the patient had spoken a few seconds previously, when Professor D. observed that the pulse had become frequent and undulating. He immediately suspended the administration of the anæsthetic. Trismus occurred; the respirations became irregular; the face turned livid, and he foamed at the mouth." The measures which were employed included the abstraction of eight ounces of blood from the jugular vein, but they were of no avail.
He only once made a feeble attempt at inspiration.92
Case 36 occurred in the practice of Dr. Wüstefeldt of Neustedt. "A young girl, thirteen years of age, had on the dorsal region a voluminous lipoma, which extended from the last dorsal vertebra to the crest of the ilium. . . . One drachm of chloroform was employed. As soon as insensibility was manifested, the operation was commenced, but scarcely had the surgeon divided the skin, when the girl, yielding to the laws of gravity, fell suddenly forwards [174/175] on her chest. Dr. Wüstefeldt, struck by the phenomenon, which he had witnessed before under similar circumstances, immediately desisted from operating, and strove to restore the patient to life; but every effort was useless, and, in the course of a few minutes, it became evident that she was dead."93
Further particulars are not given; but as the patient died suddenly, when the surgeon had scarcely divided the skin, it must be admitted that he was, in all probability, correct in attributing the event to the chloroform. The patient usually yields to the laws of gravity when only partially under the influence of chloroform, and it seems surprising that the operation should have been undertaken without placing the patient in the horizontal posture. The proper position of the patient, when a large tumour of the back is to be removed, is to be lying almost flat on the abdomen, the head being a little turned on one side, so that it rests with one ear on the pillow.
Case 37. Jane Morgan, aged fifty-nine, died whilst inhaling chloroform in the Bristol Infirmary, on January 21st, 1854. She was moderately stout, pale, but not otherwise of unhealthy appearance. "The stethoscopic indications were favourable, the beat of the heart was natural, and the air passed freely throughout both lungs; but the chest movements on the right side were not quite so free as on the left." Chloroform was ordered by Mr. Harrison, the senior surgeon of the Infirmary, with the intention of attempting to reduce a dislocation of the humerus of eight weeks standing. "Having taken no food since her breakfast, she commenced the inhalation of one drachm of chloroform, at 2 P.M., in bed in her ward, under the superin-[175/176]tendence of Mr. Hore, the house-surgeon. Nothing unusual occurring in the patient's general condition during inhalation, a second drachm, in about five minutes from the first, was poured upon the sponge, and the inhalation was continued. Almost immediately after the addition of the second drachm, the chloroform was withdrawn, as the patient's breathing became stertorous; and immediately afterwards her pulse, which had hitherto continued pretty firm, was suddenly imperceptible, the respiration ceasing at the same time. The pupils were not dilated." Various measures were promptly resorted to with the hope of restoring the patient; but there were no further signs of life, unless "some convulsive efforts of the respiratory muscles," under the application of galvanism, be so regarded.
At the examination of the body on the following day, the right pleura was found to be adherent. The lungs were healthy in structure, but gorged with dark fluid blood. There was about an ounce of fluid in the pericardium. There was a small quantity of fluid blood in each of the cavities of the heart. For the length of an inch from their commencement, both coronary arteries were much dilated, and studded with atheromatous and bony deposits. The muscular structure of the heart was examined under the microscope by Dr. William Budd, and a considerable proportion of the fibres were found in a state of incipient fatty degeneration. It was learned, after her death, that she had been subject to occasional attacks of fainting.94
Case 38. A death from chloroform occurred in the Hôpital St. Antoine, at Paris, in the spring of 1854. The subject of this was a woman aged forty, on whom M. Richard was operating for the removal of a uterine polypus. The surgeon placed the patient in the horizontal posture, [176/177] and administered the chloroform on a compress of lint. She became insensible in two minutes, having first been excited so that it was necessary to hold her. M. Richard moved the patient to the edge of the bed, gave the compress containing the chloroform into the hands of an assistant, and commenced the operation, which was likely to be of short duration. He had almost completed it, when he was apprised by an assistant, who had been set to feel the pulse; that it had ceased to beat. He sought for it himself, but found that it did not beat. The face was extremely pale; a slow respiration still continued, but soon ceased; and the measures which were used with the hope of restoring the patient were of no avail.95
At the examination of the body all the organs were found in a healthy state. The right cavities of the heart and the great veins contained a considerable quantity of blood, and the left cavities of the heart a small quantity. The blood was everywhere fluid.96
Case 39. A patient, named Mrs. Harrup, died at Sheffield from the effects of chloroform administered with the intention of removing a cancerous tumour of the left breast. The age of the patient was forty-five, and she was stated to be in good health, excepting the local affection.
"The chloroform was administered with more than the usual precautions. After the inhalation had gone on without any effect for twenty minutes, it was thought that possibly different chloroform might succeed, and one ounce was accordingly procured from the public dispensary. After the inhalation had been conducted with the fresh chloroform about twenty minutes, the usual effects of the vapour began to manifest themselves. The pulse, which was 136 before any chloroform had been given, and had [177/178] been very gradually decreasing in frequency while it improved in strength, was now about 104. At this moment muttering--half articulate delirium--came on, but ceased in a few moments, and was immediately followed by conclusive signs of the satisfactory action of the chloroform. Dr. Law now desired Mr. Wright to begin the operation but before he could do so, Dr. Law, seeing an alarming change in the countenance of the deceased, cried, 'Stop, Mr. Lewis, how is the pulse?' I replied, 'It is gone.'" After stating the means which were used with a view to resuscitate the patient, it is added that the heart had ceased to beat, and that, after a few short and laboured inspirations, life became extinct.
At the examination of the body, the cartilages of the ribs were found to be ossified. The heart and lungs were perfectly healthy, but the lungs were in a congested condition. There was an extravasation of blood in the spinal muscles, and a little blood in the spinal canal, in what part or between what structures is not stated.97
Case 40 occurred in the Lock Hospital, London, in May 1854. Walter Hollis, a tailor, aged eighteen, had been under treatment for sores within the prepuce, and these having healed, he was about to undergo the operation for congenital phymosis. He had been of dissolute habits, and exhibited a pale cachectic appearance.
"The inhaler used was a simple mouth-piece by which the nostrils are left uncovered. About two drachms of the fluid were poured into the instrument. After about six minutes inhalation, insensibility seemed to be coming on, and at this moment the pulse was ascertained to be of good volume. Nothing whatever had occurred to indicate the impending danger, when, after a few more inhalations, [178/179] the pulse suddenly failed, became quite imperceptible, and the countenance assumed a pale and leaden hue. The inhalation was immediately stopped, and attempts to resuscitate, by means of striking the chest sharply with a wet towel, applying ammonia to the nostrils, and by artificial respiration, were at once commenced. These were employed for three or four minutes before any signs of life were perceived; but, subsequently, the pulse was again to be felt, and spontaneous respiration was renewed. Artificial respiration was desisted from on the occurrence of these signs of returning life, and for upwards of ten minutes the chest continued to fill regularly, and the pulse beat at a rate of from 40 to 50 in the minute; the countenance of the patient also much improved, and even assumed a slight flush. After the expiration of, perhaps, a little more than ten minutes, however, these indications of returning vitality again disappeared, the pulse and respiratory efforts simultaneously ceased, and the countenance became deathlike. Artificial respiration and the other means were again adopted, but this time without the slightest success. . . . Post-mortem examination on the next day shewed great venous congestion within the cranium; the lungs were also somewhat congested. The heart was slightly enlarged, and the ventricular parietes were thinned; in the muscular fibres the microscope detected decided fatty degeneration. The blood was universally fluid."98
The partial recovery of the patient is a remarkable feature in this case, and it is difficult to explain why he did not recover completely. The number of the pulsations during this partial recovery is mentioned, but not their quality, and I cannot help supposing that the pulse must have been extremely weak, as well as slow, at this period. The ten minutes [179/180] during which the pulse and breathing returned is mentioned with the qualifying term of "perhaps", which leads to the supposition that it was not noted by the watch or clock, and under such circumstances of anxiety and suspense, the time might be very much overrated. The slight fatty degeneration of the heart might probably interfere with the complete recovery of the patient, after this organ had once been paralysed by the chloroform.
Case 41 took place on July 13th, 1854, in the Middlesex Hospital. The patient was a stout, muscular, and florid man, 65 years of age, on whom Mr. De Morgan was about to perform amputation at the upper part of the thigh, on account of a large malignant tumour growing from the inner side of the femur.
"Chloroform was administered by Mr. Sibley, the registrar to the hospital. Snow's inhaler was employed. The quantity at first placed in the inhaler was rather less than two drachms, and another drachm was added eight minutes afterwards. The patient inhaled the chloroform without difficulty, and went through the usual stages; at the end of about ten minutes violent spasm was induced; this continued about three minutes, and then somewhat abated. The pulse, which had risen to about 120, descended to 70, having a full, steady, and deliberate beat. The pupils, which had been much dilated, became less so. The respiration continued free and deep, but not stertorous. The colour of the face remained good.
"At this moment, which was between thirteen and fourteen minutes from the commencement of the inhalation of the chloroform, the pulse gave a few rapid and irregular beats, and then ceased. Respiration, which, as has been stated, had been going on freely, ceased simultaneously. The face became suddenly pallid and deathlike. The inhaler [180/181] was removed instantaneously, and cold water dashed on the face. Mr. Sibley immediately commenced to carry on artificial respiration, by applying his mouth to that of the patient, and inflating the lungs. The period that elapsed between the sudden cessation of the pulse and the inflation of the lungs was only a few seconds. After a few inflations, there appeared to be a slight effort at inspiration, but this was the only sign of life discovered after the syncopal attack. Galvanism was in operation within two minutes after the cessation of the pulse."
"An examination of the body was made by Dr. Corfe forty-eight hours after death. In the head nothing particular was discovered; the brain was firm, and rather more vascular than natural; the blood in the sinus was partly coagulated; the heart was rather larger than natural, and was extremely loaded with fat, especially on the right side, where fat formed three-fourths of the thickness of the wall of the ventricle; the muscular tissue was extremely pale and soft, and exhibited both to the naked eye, and the eye assisted by the microscope, an extreme degree of fatty degeneration; the blood in the cavities of the heart was firmly coagulated; on both sides it was almost purely fibrinous; the clot on the right side was larger than on the left; a fibrinous clot extended down the aorta." 99
I do not know how the bibulous paper was arranged in the inhaler in this instance, nor whether the inhaler was used with a view to regulating the amount of vapour in the inspired air. The proportion of vapour must have been small during the first ten minutes, as the patient became so slowly insensible; and judging from the result, we must conclude that the proportion was large just before the accident. The firm coagulation of the blood and separation of the fibrin were probably owing to the galvanism which [181/182] was so promptly applied. I found the fibrin separated from the colouring matter of the blood in the cavities of the heart of a cat, in which shocks of electro-magnetism had been sent through the chest just after it had been killed with chloroform.
Case 42. A man died whilst inhaling chloroform in University College Hospital on October 11th, 1854. The patient was a shoemaker named George Sands, aged 39, and of rather bloated aspect. He inhaled chloroform whilst Mr. Erichsen was endeavouring to introduce a catheter, and had the intention of puncturing the bladder if not successful. The patient was made insensible, and the chloroform was left off, but was reapplied on account of the patient making some expression of pain. "Probably about two minutes of the second inhalation had elapsed, when the man became profoundly insensible, and began to snore with a peculiar and very profound stertor. His face at this time was suffused and flushed, and the inspirations were drawn at rather prolonged intervals. Mr. Erichsen's attention was at once excited by these symptoms, and, desisting from the use of the catheter, he immediately commenced dashing the patient's face and chest with water. The chloroform had, of course, been removed. In the course of about a minute, the noise with the breathing gradually lessened, and it became apparent that the respiration was ceasing altogether. Mr. Erichsen now put his finger into the patient's pharynx, and dragged forwards the root of the tongue; at the same time attempting artificial inflation of the lungs, by applying his own mouth to that of the man. The latter plan did not appear to succeed well, and was almost immediately substituted by the more usual mode of artificial respiration, by compression of the chest, which was kept up most vigorously. The man's pulse had been felt by the adminis-[182/183]trator (Mr. Carnell) to be still beating some little time after the commencement of the alarming symptoms and the cessation of respiration. Artificial respiration had been employed for about four minutes, when the man, whose countenance had meanwhile retained its colour and an expression of yet remaining life, began to breathe again. A very short intermission of artificial assistance having been made, he drew spontaneously three or four inspirations; but, as each successive one was more feeble, the artificial aid was at once recommenced. About five minutes from the commencement, the galvanic apparatus was got in readiness and applied. It produced, however, no benefit; and from this time the patient lost colour in the face, and was evidently dead. . . . The form of inhaler which had been employed was the one in ordinary use at this hospital, viz. a folded piece of lint. The administrator's hands and the patient's face had been covered during the inhalation by a towel."100
At the examination of the body seventy hours after death, extensive fatty degeneration of the heart was met with. The cavities of the heart were empty, owing, no doubt, to the artificial respiration.101
The above case differs to a certain extent from those previously quoted, inasmuch as the first symptoms of danger were those of profound coma, and of threatened death by apn?ìa, as a consequence of the action of the chloroform on the medulla oblongata and nerves of respiration. In addition to this cause of danger, however, the chloroform present in the lungs at the moment when the inhalation was discontinued must have acted directly on the heart, or the prompt assistance of so able an authority on asphyxia as Mr. Erichsen, the moment the breathing was suspended, would surely have restored the patient. [183/184] The mode of death, although not exactly the same as that in Experiment 24 (page 110), differs from that in the previous experiment, where the heart's action was good and distinct after the breathing ceased; it resembles the mode of dying in many animals that I have killed with chloroform; being, in fact, a combination of death by apn?ìa and cardiac syncope, which generally occurs when the quantity of vapour in the respired air is intermediate between that in Experiments 23 and 24, or somewhere between 5 and 10 per cent.
A great peculiarity in the way in which chloroform was administered in the case we are considering was that the head and face of the patient were covered by a towel, under which the lint wetted with chloroform was held. The countenance and state of respiration could not be observed in this mode of giving the chloroform; the person administering it had to depend almost entirely on the pulse; and, except for this cause, there is every reason to conclude that the chloroform would have been withdrawn in this instance in time to save the patient. It was not apparently till a peculiar and very loud stertor attracted the attention of the operating surgeon himself, that the inhalation was discontinued, and the face was already suffused.
This plan of administering chloroform with the head and shoulders of the patient covered with a towel, was introduced by Mr. Clover, who was for several years a resident officer of the institution; and it is but right to state that it led to no accident in his hands; in those of his successors it was, however, less successful; three accidents having occurred in a little more than a year and a half. I much regret to find that Mr. Erichsen recommends this method of giving chloroform in the edition of his work on surgery recently published. [184/185]
Case 43 occurred in Guy's Hospital, on December 5th, 1854. The patient was a woman whose leg Mr. Birkett was about to amputate on account of malignant ulceration. She gave her age as fifty-six, but appeared ten years older. "In each eye was a fairly marked arcus senilis, but the woman was not known to have suffered any symptoms referable to thoracic disease. . . . The administration of the anæsthetic was conducted by Mr. Bryant, the inhaler used consisting of a fold of lint, rather larger than an out-spread hand, and protected on its back by a piece of oiled silk to prevent wasteful evaporation. . . . In the first instance, about a drachm of the fluid was poured upon the lint. The patient inhaled it kindly; and, after about two minutes, another drachm was added. A stage of excitement now followed, during which the limbs required to be held. Insensibility was just fully established, and Mr. Birkett was on the point of commencing the operation, when Mr. Callaway, who was compressing the femoral artery, exclaimed that the pulse had suddenly ceased entirely. The wrist was examined, and the same found to be the case. Almost immediately afterwards, a long-drawn inspiration, attended with a deep sighing noise, was observed. For two or three breaths the cheeks puffed out during expiration; the respiration next fluttered, and then ceased. Mr. Birkett at once put his finger into the patient's mouth, and drew forward the tongue, artificial respiration being meanwhile commenced by assistants by means of compression of the chest. A few slight inspirations were attempted by the patient subsequent to the commencement of the artificial assistance; but they did not continue, and no sign of vitality was ever afterwards shown. . . . It must be noted, that the woman had been very pale both before and throughout the exhibition, and that no change in her appearance was perceived when the alarming symptoms occurred, excepting that the superficial veins of [185/186] the neck and temple became distended with blood. The cessation of the pulse was most sudden. Mr. Callaway stated that it was not preceded by the least premonitory fluttering, the stroke having been good one beat, and entirely wanting the next. This order of symptoms was of course suggestive of death beginning at the heart (cardiac syncope), the cessation of the functions of the nervous system having been markedly subsequent to that of the circulation. . . .
"Autopsy, twenty-four hours after death (conducted by Dr. Wilks). The corpse was much emaciated, and the rigor mortis imperfect. The lungs were much congested with fluid blood, which ran out after incision of their substance. The heart was of normal size, but soft and flabby; its left side was nearly empty, the right being distended with fluid blood. The left ventricle was of good thickness; its muscle of a deep colour, not encroached on by fat, or in the least mottled, the only observable departure from a healthy state being its flabbiness. The right ventricular wall was very thin, the subserous fat having in some parts almost taken the place of the muscular tissue. The layer of the latter, however, although much thinned, had still a good colour, and did not appear to the naked eye as degenerated, an observation which may apply also to the carneæ columnæ. The liver was in an early stage of cirrhosis, and the kidneys were both of them mottled, and contained numerous small cysts in the external part. The brain was rather paler than usual, its convolutions appeared shrunken and atrophied, and there was a quantity of serous fluid in the arachnoid sac and in the ventricles. There was general atheromatous disease of the arterial system, both in the head and other parts of the body. The blood was universally fluid, and of a dark colour."102 [186/187]
As far as could be estimated, the time occupied by inhalation was about three minutes in this case.
Case 44 occurred at the Royal Ophthalmic Hospital, on April 10th, 1855, in a man on whom Mr. Bowman was about to perform excision of the left eyeball. The patient, named John Cannon, was forty years old, and was moderately stout, florid, and healthy-looking. He had generally led a temperate life. The disorganisation of the eye was the result of injury.
"The inhaler used was the one devised and recommended by Dr. Snow. . . . The administration was intrusted to Dr. Playne, of King's College Hospital. In the commencement of the inhalation, the valve of the mouthpiece was so turned as to admit an abundant supply of air, a point to which Mr. Bowman directed personal attention. During the first four minutes (more or less) nothing unusual occurred. Dr. Playne, who had his finger on the pulse, had noticed that it had rather increased in fulness, and was of good volume. Rather suddenly, however, just as the anæsthetic appeared to be producing its effect, symptoms of excitement occurred. The eyes became fixed and staring, the arms outstretched and rigid, and the face contorted. It was now impracticable to feel the pulse, on account of the tossing about of the arms but, as is usual in such conditions, the respiration was noticed to be all but, if not quite, suspended by the spasmodic fixture of the chest. The inhaler was at once removed, and the face and chest of the patient dashed with cold water. Almost immediately after, as the respirations had become extremely feeble and sighing, Mr. Bowman commenced practising artificial breathing, by the application of his own mouth to that of the patient. By this means, the chest was made to fill very completely, and the process was kept up almost without intermission for from five to [187/188] eight minutes. During the first three or four minutes after the alarm began, the patient continued at times to make slight sighing efforts at voluntary inspiration, and the case was not thought, by those looking on, to be by any means hopeless. At length, however, these finally ceased, and from that time it was apparent that the man was dead. . . . At the first opportunity which occurred for examining it after the spasmodic struggling had commenced, the pulse was found to be extinct, and it remained so ever after, although there were, as stated, feeble efforts at inspiration. The patient's countenance changed somewhat during the treatment, but was mostly suffused and congested."
At the examination of the body forty-eight hours after death, "the sinuses, and the veins of the brain generally, were much congested, and there was some œdema of the brain substance. The heart, excepting some slight deposits on the curtains of the mitral valve, was healthy. Its muscular substance was easily lacerable. The right ventricle contained a considerable quantity of fluid blood, the left was nearly empty. There were some pleuritic adhesions, and the lungs generally were congested, being also in some parts full of air. The blood in every organ examined was fluid, and without trace of coagulation."103
It does not seem that the inhaler used in this case was employed with the object for which it was contrived--that of regulating the amount of vapour in the inspired air; and I do not know whether the bibulous paper was arranged properly in the interior.
Case 45. On September 8th, 1855, a lady, aged twenty-nine, the wife of a physician, died suddenly whilst inhaling chloroform for the relief of facial neuralgia. I was sent for [188/189] when the accident happened, and arrived twenty minutes afterwards. I found the deceased lady without any sign of life. The face and lips were very pallid. The husband was performing artificial respiration by mouth to mouth inflation of the lungs, and alternate pressure on the chest, and I assisted him in this for a long time, though with no hope that any thing could be of service. Dr. Barker, of Grosvenor Street, arrived soon after me, and assisted in the same measures. An inhaler was employed in this case consisting of a face-piece, like the one above delineated in this work, and a bent metal tube lined with bibulous paper. Two quantities of ten minims each had been inhaled, with some relief to the pain, and without causing unconsciousness when the inhaler and the chloroform were put away in a closet; but the patient begged to have more chloroform, in order to be completely relieved of the pain, as she had been on a previous day. Ten minims more chloroform, as I was informed, were put into the inhaler, and the patient, being seated on a sofa, began to inhale very eagerly, but had no sooner commenced than she gave a sudden start, as if taken in some kind of fit. Her husband laid her on the floor, but she evinced no further signs of life.
There was no inspection of the body.
The only explanation which the case admits of is that, in her eagerness to get relief, the patient took one or more inspirations of air very highly charged with vapour. The symptoms were those of death by cardiac syncope.
Case 46 occurred in the practice of Dr. Roberts, a surgeon-dentist of Edinburgh. The patient was a lady, thirty-six years of age, to whom Dr. Roberts had administered chloroform on four previous occasions within a twelve-month. Dr. Roberts says the chloroform was administered in the usual way, by which he means on a handkerchief. [189/190] He says: "Mrs. H. had only taken about nine or ten inspirations, obtaining but a partial influence of a quantity short of Ʒiss [one and one-half drachms] poured out from the bottle, and inhaling it for a space of time certainly less than a minute, when she said, 'You must not operate until I am quite insensible'; and again, 'I am not over yet'; and immediately, even while speaking, she gave a convulsive start, and with a stertorous inspiration, and with the eyes and mouth open, sunk to the floor." Dr. Simpson was sent for, and arrived within five minutes. Artificial respiration was resorted to, and after it had been applied for a time, there were a few spontaneous inspirations, and the pulse, it is said, could be perceived at the wrist; but these symptoms of reviving animation disappeared.
At the examination of the body, the right cavities of the heart were found gorged with blood. The walls of the right ventricle were thinner than natural, and affected to a certain extent with fatty degeneration.104
A paragraph was inserted in some of the Edinburgh newspapers, and forwarded by Dr. Roberts to the Lancet,105 in which it was implied that death in this case was not caused by the chloroform. It is, however, like the preceding case, a well marked instance of the sudden and fatal action of this agent.
Case 47. A sailor, aged thirty, died whilst inhaling chloroform in St. Thomas' Hospital, in October 1856, preparatory to having some necrosed bone removed from one of his fingers. "He did not appear to be in robust health; still there was no obvious reason against his having the chloroform, which was accordingly administered as follows. One drachm was poured on a sponge folded between two thicknesses of lint, and this held at a little distance from [190/191] his mouth, while he was sitting in a chair. He appeared to be going off very comfortably, when the chloroform was left off for from half a minute to a minute, and then resumed. He now began to raise his hands and tremble, and kept spitting in the lint, and appeared as if about to vomit. Suddenly he was violently convulsed through his whole frame, as if in an epileptic fit. The chloroform was at once discontinued, and he was laid in a semi-horizontal posture. The convulsion only lasted for a few seconds, and when it had ceased he began to breathe with effort and puffing of the lips, and almost immediately to gasp irregularly. His pulse was almost imperceptible and intermittent. Artificial respiration was at once performed by alternate compression and relaxation of the walls of the chest, the tongue being held out of the mouth by the forceps. Ammonia was applied to the nostrils, and cold water dashed in the face, and in about a minute he rallied so as to breathe without assistance, but in a few seconds he relapsed, and could not be recovered.
"At the post-mortem examination there was found to be fatty degeneration of the heart, liver, and spleen, and the membranes of the brain were thickened. The lining of the ventricles presented a peculiar pitted appearance, apparently from inflammatory deposit. The brain itself was pale."106
It was ascertained after the man's death that he had been of intemperate habits, and had an attack of delirium tremens three weeks previously. In the report of this case in the Association Medical Journal, the following is the account of the appearances met with after death. In the autopsy in the present case, which we observed with particular care, the brain was in a state of œdema and bloodlessness, very like the brain in a patient who died from chloroform in the Ophthalmic Hospital. The liver was [191/192] fatty; but the heart seemed the very model or type of the healthiest kind of heart. All the other organs were also healthy."107
Case 48 is related by Mr. Paget as follows. "I am anxious to place before the profession, at the earliest opportunity, a narrative of a case in which chloroform proved fatal in my private practice.
"The patient was a boy, nine years old, of delicate constitution, and of nervous, timid disposition; but with no indication of any organic disease, except that for which the operation was to be performed: namely, a tumour of the scapula; for which it was proposed to remove the greater part of that bone.
"At half-past eight A.M., on February 28th [1856], after the patient had passed a night of sound sleep, the chloroform was first administered in a room adjoining that in which the operation was to be performed. He was alarmed at the thought of being put to sleep, and of what would then be done, and was very averse from taking chloroform, but he was persuaded to inhale it; and, though not without resistance, yet with less than is commonly made by patients of the same age, he was brought under its full influence in about three minutes. He sat in bed during the first few inspirations, and after these, was recumbent. It was observed that two or three deep inhalations were quickly followed by complete insensibility; and the next few inspirations were stertorous. He was at once carried, in the horizontal posture, into the room, and laid on the table, arranged for the operation.
"Three or four minutes passed while we were arranging his position and his dress, and while I was pointing out to those who were to assist me the proposed plan of operation. [182/193] During this time the influence of the chloroform so far passed off, that he became sensible, displaced his coverings and pillows, said something expressive of discomfort, and vomited a small quantity of frothy fluid. (He had taken no food. since the previous night, when he had had a good supper.) A very small quantity more of chloroform was slowly inhaled, and he became again nearly quiet, and was again placed on his side. I was on the point of commencing the operation, but as he again, by movements, indicated some degree of sensibility, and changed his posture, about forty drops more of chloroform were poured on cotton wool, inclosed in a fold of lint,--an inhaler, with the chloroform on sponge, having been previously used. The lint was held, about half an inch from the face, by Mr. Thomas Smith, my usual assistant in operations. The patient inhaled lightly for a few times, then made one long inspiration, and appeared to pass at once into deep sleep. Except that he thus appeared to come suddenly under the full influence of chloroform, no external change was visible; but, a few seconds later, his pulse, which had been carefully watched, and had been to this time normal, suddenly began to beat very quickly; then it ceased for two or three seconds; then beat rapidly several times, with a kind of flickering movement; and then ceased to be perceptible.
"Just before this change of the pulse was observed, the chloroform had been withdrawn. The one deep inspiration was followed by a few stertorous breathings, but after these he breathed naturally, his complexion and features showed no change, he seemed only calmly asleep, and in this state he continued breathing naturally, and with no change in his appearance, but pulseless, for at least a minute. Then his breathing became less frequent, and seemed as if it might soon cease; his face grew pale, and his lips very slightly livid.
"With the help of cold water sprinkled on his chest and [193/194] face, and cold air blown on his face and throat, he was raised from this state of defective breathing in about two minutes, and again breathed deeply and freely, though slowly, (probably about twelve times in the minute.) He thus breathed for two or three minutes, and during this time the lips, and the pale or slightly livid parts of the face, became pink again, and though no pulse could be felt at the wrists, the heart was heard acting. During this time, also, some wine and brandy were poured into the mouth, and passed down the œsophagus, but without any evident movements of swallowing. His breathing again became gradually infrequent and feeble. Cold air and sprinkling with water, frictions and percussions of the chest, scarcely increased the breathing, and in less than two minutes it ceased. Artificial respiration, by the method of Dr. Marshall Hall, was immediately employed, and many times during the first five minutes of its employment the artificial inspiration obtained, when turning the body over to its side, was followed by a distinct, and sometimes even a full muscular inspiration. But at the end of about five minutes, these signs of life ceased, fæces escaped, and no more indications of life appeared, though the artificial breathing, the friction of the limbs, and other means for resuscitation, were continued for twenty or more minutes.
"I refrain, at present, from all comments on this case. Only, I wish to call particular attention to the fact that good breathing was maintained, and, after a suspension, was renewed, long after the heart had ceased to act with sufficient force to produce a pulse at the wrist. And I would add, that this narration is sanctioned and considered to be exact, by the four gentlemen who were to have assisted in the operation, and to whom I am greatly indebted for their counsel and assistance in the greater difficulty that we had to cope with."108
Case 49. This case occurred in the Liverpool Infirmary on April 5, 1857, and is related by Mr. Allan, the resident officer who administered the chloroform. The subject of the case was a labourer, aged 35, on whom Mr. Bickersteth was about to perform amputation of the thigh on account of gangrene following the ligature of the femoral artery. He had inhaled the chloroform six days previously without ill effects, when the femoral artery was tied for popliteal aneurism. On the day of the accident, he was first rendered insensible in the ward by chloroform poured on a piece of lint which was held a short distance from the nose and mouth. Having partially recovered during his removal into the operating theatre, the chloroform was reapplied, and Mr. Allan relates what occurred as follows: "About half a drachm of chloroform was now poured on some lint, which was held to the nostrils, and he then became fully under the influence; respirations good; pulse frequent, feeble. The operation was about to be commenced, and I was pouring about twenty minims more chloroform on the lint, (having pronounced the patient to be in a fit state,) so as to be ready to give him some more as occasion required, but had not applied it, when, turning round, I noticed something peculiar in his general appearance, and, on lifting up the eyelid, found the pupil dilated, and the lid did not close over on the removal of the finger; the eyes were slightly turned up. I at once felt for the temporal artery, but there was no pulsation, and none detected at the left wrist; the respirations had almost ceased. The head was lowered, cold water was dashed on the face, and the abdomen struck with the palm of the hand; the finger thrust into the mouth (there was no action of the heart felt); the legs were elevated, and a wet towel was dabbed over the epigastrium. After one or two blows, the respirations became better, and seemed good, and in about two minutes a pulse was [195/196] felt at the wrist. This continued between two and three minutes, the respiration being good. His pulse then began to fail, and in about a minute more the respirations were less. The tongue was seized with a pair of forceps, and drawn forwards, and artificial respiration tried, and ammonia held to the nostrils; but he was becoming livid in the face, so the Ready Method was at once adopted, and this produced apparently a few natural respirations. But the pulse had gone, and in about two minutes more there was no breathing save artificial. About the time that the pulse stopped, there was a convulsive movement of the muscles of the leg, and a slight clamminess of the skin succeeded. The Ready Method was continued for half an hour, and galvanism tried, but without avail. From the time he was placed on the table to his death, or the cessation of natural respiration, about ten minutes elapsed."
The writer adds: "He apparently sank from syncope, or cessation of the heart's action, for his respiration had been good just before he changed, and it continued for a second or two, though faint, when the pulse had stopped; and after the respiration had been restored, and was very good, the pulse was very feeble, and ceased two minutes before the respiration."
At the autopsy on the following day, the brain was found to be healthy, tolerably firm, and pale; the lungs were healthy; the right cavities of the heart contained some fluid blood, which afterwards coagulated on exposure, and a small clot. The left cavities also contained some blood. The muscular tissue of the heart had an unhealthy look, and very readily tore, but no oil globules were discovered with the aid of the microscope.109
Case 50 occurred in King's College Hospital, August 7th, [196/197] 1857. The following is the account of the case furnished by Mr. C. Heath, the House-surgeon:
"The patient (Ann Stoner) was a female, aged seventeen, under Mr. Partridge's care, with syphilitic warts and mucous tubercles. She was admitted July 8th, and had had chloroform administered twice, in order that the sores might be touched with nitric acid, and, on both occasions, not the slightest ill effect was produced. On Friday evening last, chloroform was again administered for the same purpose; only a drachm was put into the inhaler (Snow's), and as soon as she became unconscious the inhaler was removed, and the acid applied. I and my assistant (who administered the chloroform), then went to see another patient in the same ward, and then washed our hands, during which time the patient was moving her legs about much as they do when recovering, and in addition she made water over the bed. I gave directions to the nurse to apply a poultice as usual, and left the ward, having been up to the bed first without noticing anything unusual about the patient. In a few minutes the nurse came down for some medicine for another patient, and mentioned. that this one was looking very pale: I sent up Mr. Liddon to see her at once; he found her pale and senseless, dashed some water over her, and called me, and I went up immediately. I found her pulseless and cold, and immediately commenced artificial respiration (Marshall Hall), and sent for the galvanic battery; this was brought and applied without effect, and the artificial respiration was continued for twenty-five minutes without the slightest effect being produced."110
I was present at the examination of the body on the following day. The mouth was sore and swollen f[r]om the effects of the inunction of mercury. There were a few drachms of clear serum in the pericardium. The heart was [197/198] large for the size of the patient. There was a patch of organised lymph on the pericardium, covering the left ventricle. The right cavities of the heart were full of dark fluid blood, and the left cavities contained a little. The mitral valve was much thickened, but the other valves were healthy. The lungs were healthy, and not much congested. The brain was healthy. The patient had suffered from acute rheumatism before entering the hospital.
It will be observed that the pulse is not mentioned in the above case, until its absence is alluded to, when the patient was already cold, and the breathing is not alluded to throughout the account; indeed, it is not known when the patient died. She was alive after the application of the nitric acid, as she was observed to move her legs, but further than this there is no clear evidence.
It is perhaps an open question whether this patient died at once from the direct effects of the chloroform, or whether she died after partially recovering and going on favourably for a time. The account would, at first view, seem to favour the latter opinion, but it is not corroborated by any other case. Patients have been partially recovered from the effects of an overdose, without being entirely restored, and others have sunk after great operations, attended with hæmorrhage, when the effects of the chloroform had more or less subsided, but there is no instance of a patient going on favourably, and partially recovering from the influence of the vapour, and then dying suddenly without any other known cause. Patients have occasionally become faint whilst recovering from chloroform, more especially if they remain in the sitting posture, but in those cases the right side of the heart is probably insufficiently supplied with blood; whilst, in the case under consideration, the patient was lying, and the right cavities of the heart were found full after death, the serum in the pericardium showing that [198/199] they had probably been distended when death took place. If Mr. Heath had made any observation which enabled him to say that the patient was really alive, when he went up to the foot of the bed, before leaving the ward, it would decide the question, and show that death did not take place at once from the direct effects of the chloroform, but he only makes the negative remark that he did not notice anything unusual about the patient.
I had an opportunity of examining the particular inhaler employed, and found that it was so arranged that the vapour might be breathed from it in much greater proportion than would be safe, if precautions were not taken to leave the expiratory valve a considerable way open, especially when the high temperature of the weather at the time is taken into account.
The foregoing cases comprise all the instances I have seen recorded in which death appears to have been occasioned by the administration of chloroform, and not by other causes in operation about the same time. A few additional cases have indeed been referred to by different authors where death was probably caused by chloroform, but as I do not find that the details have been published, I cannot make them available in an inquiry respecting the cause and prevention of these accidents.
In June 1852, Dr. Simpson alluded in the following terms to an accident from chloroform which had occurred near Glasgow:--" In this instance, chloroform was given by the practitioner for tooth extraction but, I am sorry to add, none of the parties present were at the time in a condition to give any satisfactory evidence."111
A person, named Breton, a dealer in porcelain, died in Paris, in the early part of 1853, immediately after a few [199/200] inspirations of chloroform, which was administered with the intention of removing a tumour of the cheek. An action was brought against Dr. Triquet and M. Masson for causing death by imprudence in this case; and at the trial which ensued, various interesting opinions were given, and the accused practitioners were ultimately exonerated.112 I have not, however, met with any record of the symptoms which occurred in the case.
In relating the case of death from chloroform, which occurred in his practice, to the Medical and Chirurgical Society of Edinburgh, Dr. Roberts referred to another death from chloroform in tooth-drawing which took place in the neighbourhood from which his own patient came, just previously to October 1855; but I have not met with any account of the case so alluded to. Dr. Mackenzie of Kelso also alluded in the same Society, in the following year, to a death from chloroform which had occurred at Coldstream, and I do not know whether this was the case to which Dr. Roberts had alluded, or a fresh one. One of the surgeons to the hospital at St. Louis, who was lately visiting the medical institutions of London, informed me that there had been three deaths from chloroform at his hospital out of between six and seven hundred operations in which it had been administered. I did not learn the particulars of those fatal cases.
There have been several cases in which persons have been found dead after inhaling chloroform when no one else was present, either for toothache or some other affection, but I have not included such cases in the above list, as they throw no light on the way in which death is occasioned. The simple way to avoid such accidents as those just alluded to, is for persons to abstain from inhaling chloroform, when no one is by to watch its effects. [200/201]
Several deaths have been attributed to chloroform which were due to other causes, or where the cause of death is a subject of great doubt. A gentleman, named Walter Badger, twenty-two years of age, the son of one of the coroners for the county of York, died instantly at Mr. Robinson's, the dentist's, in Gower Street, on June 30th, 1848, whilst commencing to inhale chloroform with the intention of having some teeth extracted. The inhaler employed consisted of a face-piece to enclose the mouth and nostrils, and containing a sponge on which the chloroform (Ʒiss [one and one-half drachms]) was placed. This, according to the evidence of Mr. Robinson and his female servant, who was present in the room, was held not nearer than an inch and a half from the face for less than a minute, and the patient made the remark that the chloroform was not strong enough; Mr. Robinson requested him, as he had done before, to have the operation performed without chloroform, but he again declined; and Mr. Robinson then took away the face-piece and asked his servant to reach the bottle, intending to put more chloroform on the sponge, to replace that which he believed had been lost by evaporation. Just after removing the face-piece, and before any fresh chloroform was poured out, the head and hand of the patient dropped, and he did not show any further sign of life.
I found, on making trial of the kind of inhaler which Mr. Robinson employed, that it is impossible to inhale enough of the vapour to produce any appreciable effect, unless it is applied so as to touch the face. At the distance of an inch no effect is produced, even in five or ten minutes; and therefore I expressed my opinion, soon after this accident, that it was not caused by the chloroform, which properly speaking the patient did not inhale. [201/202]
A consideration of the symptoms in this case confirms the view that the death was not caused by chloroform. In six of the fatal cases related above, death took place instantaneously, without insensibility or any of the usual effects of chloroform having been produced; but the mode of dying was not the same as in Mr. Robinson's patient. In Case 4, that of Madlle. Stock, the patient said "I choke", and tried to push away the handkerchief; then there was embarassed breathing and foaming at the mouth. In Case 11, that of Madame Labrune, the fatal attack followed immediately on a full inspiration of chloroform, and there was an immediate alteration of the features, and a convulsive rolling of the eyes, amongst other symptoms. In Case 14, the young lady stretched herself out, and frothed at the mouth, at the moment of the fatal attack, and the face became livid. In Case 26, that of Madame W., who died at Ulm, the voice, when answering the question about singing in her ears, was trembling and thick; she stretched out her limbs, and the face became bluish. In Case 45, that of the wife of a medical man, and in 46, that of Dr. Roberts's patient in Edinburgh, there was a convulsive start at the moment of the sudden death. It thus appears that when the heart is suddenly paralysed by an overdose of chloroform, before the patient is rendered insensible, there are usually some symptoms as if of a violent shock or injury. After complete insensibility is induced, the heart may be suddenly paralysed by chloroform, as is shown by numerous cases, without this spasmodic action; and it would perhaps be premature to deny that a patient might die thus quietly without being first made insensible; and the nature of the death in this particular case must be chiefly decided by the physical fact that the patient could not have inhaled enough chloroform to produce an appreciable effect of any kind, much less to cause sudden death. [202/203]
At the inspection of the body, the liver was found so much enlarged that it weighed eight pounds, and it encroached very much on the chest. The walls of the left ventricle of the heart were found thinner than natural, and the muscular tissue was interspersed with fatty degeneration. There was blood in the right auricle and in both ventricles. In the ventricles it was partly coagulated. The brain presented nothing abnormal.113
It is probable that the immediate cause of death in this instance was fear. The patient had been told in the country that it would be unsafe for him to take chloroform, and yet he could not summon resolution to undergo the operation without it. Mr. Robinson unfortunately allowed his patient to remain seated in the operating chair; and it was only when Dr. Waters had been sent for and arrived from a neighbouring street that he was laid on the floor.
I was present on one occcasion with Mr. Peter Marshall at the examination of the body of a woman who died suddenly of fright in consequence of a fire in the next house to that in which she lived, and it is worthy of remark that we found exactly the same diseased conditions as those which were found in Mr. Robinson's patient; viz., great enlargement of the liver, displacing the viscera of the chest, and fatty degeneration of the heart. A young man, aged twenty-four, died suddenly of syncope, on June 25th, 1848, at the Hospital Beaujon, at Paris, whilst M. Robert was performing amputation at the hip joint, the thigh bone having been broken into splinters by a bullet during the conflict in the streets of Paris. The patient was in a state of great depression, both physical and moral, before the operation; and it is most likely that he sank under the combined effects of the injury and the operation. [203/204]
Another patient had the neck of the humerus broken by a ball in the same conflict; he was much reduced by hæmorrhage and gangrene of the wound; M. Malgaigne performed disarticulation at the shoulder joint; a fresh inhalation took place to enable him to search for the ball, and the patient sank and died during the last incisions. This patient also most probably died from the effects of the operation added to those of the previous injury and loss of blood.
A woman died in Paris, 1848, after removal of the breast. The operation was finished, and the chloroform had been left off some time, and the patient had become conscious, when on raising her into a sitting posture, in order to apply a bandage, she suddenly expired. Although the chloroform was blamed in this instance, death evidently took place by the ordinary kind of syncope, which arises from the heart not being supplied with blood, and which may be called anæmic syncope, in contradistinction to cardiac syncope, which begins at the heart itself, when properly supplied, or even when distended with blood.
A child, aged twelve years, died in the hospital at Madrid in 1849, during amputation of the leg after violent tetanic rigidity.114 Death was attributed to the chloroform which had been inhaled, but no further particulars are given, and it is not stated whether or not there was any unusual hæmorrhage, or other cause, which would explain the fatal event.
Dr. Aschendorf has attributed the death of a child a year old to chloroform.115 The child had a nævus on the face and neck, which extended from the zygoma to the os hyoides, and from the external auditory meatus to the [204/205] maxillary fossa. No one had been willing to undertake its removal. Dr. Aschendorf operated on the nævus at three different times, by means of seton threads. These operations were performed under the influence of chloroform. The tumour was reduced one-third part in size by these means, and eleven weeks afterwards Dr. Aschendorf determined to extirpate it. The chloroform was administered as on the former occasions, by placing six drops on some tow in a cup. In about ten minutes, as the child cried a little, three drops more of chloroform were used for inhalation, and in about eight minutes more the operation was concluded. "On raising the child it laid its head on one side, convulsive twitches of the face were observed, with distortion of the eyeballs and dilatation of the pupils. For one moment the arms were stretched out stiff, then again they were relaxed, and fell as supple as the rest of the body. Death quickly followed--only one pulsation of the heart and a single rale with the expiration being perceived."
There can be no doubt of this being a case of death from hæmorrhage, after the direct effects of the chloroform had subsided. Dr. Aschendorf says the quantity of blood lost was about two tablespoonfuls; but it would be necessarily removed by sponges during the operation, and there would be no means of estimating the quantity. The child was probably in a state of syncope during the latter part of the operation, as it would not remain insensible to the knife for eight minutes from a single application of chloroform.
On September 15th, 1852, a patient died to whom I was administering chloroform whilst Mr. Cæsar Hawkins was performing lithotrity. He was a gentleman from the country, aged seventy-three; he was tall and stout, he had a weak intermitting pulse, and a well marked arcus senilis in each cornea. He had inhaled chloroform five or six [205/206] times, between May 1850 and May 1851, for the same operation, when under the treatment of another surgeon, and it always acted favourably. In the first week of December 1851, Mr. Hawkins, performed the operation of lithotrity twice, when the chloroform was administered by Mr. Geo. D. Pollock. On the second of these occasions he became faint during the operation whilst under the influence of the chloroform, but recovered from the faintness before its conclusion. He again fell into a very alarming state of syncope a few minutes after the conclusion of the operation, but rallied, and vomited the breakfast which he had taken a little time before. I first administered the chloroform to this patient on December 15th, 1851, eleven days after the above occurrence. Mr. Hawkins and I were inclined to think that the alarming syncope on the previous occasion might have been connected with the sickness which occurred. It was my firm belief that the patient had fatty disease of the heart but I did not see any great objection to the chloroform on that account, as I had frequently given it in similar cases, and always with a favourable result. On this occasion (December 15th) he inhaled the chloroform before breakfast. Its effects were quite satisfactory, and it was not accompanied or followed by any unpleasant symptoms whatever. The operation was repeated four days afterwards, when I again exhibited the chloroform with like favourable results. After this the patient went back to the country relieved from his stone. He came back, however, in the autumn of 1852, with a return of his complaint, and I was again requested by Mr. Hawkins to assist him by giving the chloroform on September 15th.
The patient became insensible, without any excitement or struggling, in the course of three or four minutes, and the operation was commenced. A little more chloroform was [206/207] administered two or three times during the operation, in order to keep up the insensibility. After a few minutes had elapsed, I observed that the face and lips of the patient became pale. At this time he had not inhaled any chloroform for about two minutes. Immediately afterwards, however, his face became red, and he made straining efforts with the muscles of respiration, as if he were beginning to feel the operation. To prevent his becoming altogether sensible, therefore, I commenced to give him a little more chloroform, with the valve of the inhaler about one third open, as on the former occasions. He had only taken two or three inspirations, however, when the breathing ceased. He appeared to be merely holding his breath, as sometimes happens during the exhibition of chloroform, and I expected that he would begin to breathe again in about a quarter of a minute. In the meantime, I endeavoured to feel the pulse in the temporal artery, but did not perceive any. Instead of the breathing recommencing at the time I expected, the countenance became suddenly pale, and a little afterwards rather livid. I applied my ear over the region of the heart, but could not hear any sound. After a few seconds, however, the patient took a rather deep inspiration, and immediately after this I was pretty sure that I heard the heart beating very feebly and rather frequently, but only for a few seconds, after which no sound could be heard. There were one or two more very feeble inspirations at intervals of about a quarter of a minute, after which there were no further signs of life. As soon as the patient had entirely ceased to breathe, artificial respiration was performed, but no sign of returning animation appeared.
At the examination of the body fifty-two hours after death, the heart was found to be larger than natural, and there was a good deal of fat on its surface. Its right cavities contained air or gas, probably resulting from the [207/208] partial decomposition of the blood. The right ventricle was dilated, and its walls were very thin. At one place, near the apex, they were extremely thin. The left ventricle was also dilated, but its walls were of the proper thickness. They were, however, like those of the other ventricle, very soft and friable. There was a calcareous incrustation on one of the aortic valves. There was scarcely any blood in the heart, but its lining membrane was stained in places, showing that blood had been present after death.
Mr. Pollock and the late Mr. W. F. Barlow examined the structure of the heart under the microscope, and the latter gentleman furnished me with the following account of the examination:
"Many of the fibres have been converted into fat completely; in others, fatty degeneration was beginning. The degeneration, which was in various stages, appeared very general. The fasciculi were broken up, here and there, into masses of small irregular fragments, as they may be found frequently in hearts of this kind. Some large fat globules lay between and upon the fibres. A few fibres showed their transverse stria plainly, and made the changes in the others look the clearer. On the whole, it may be said that the structure of the organ was greatly damaged, and that its action, consequently, was liable to cease suddenly from slight causes."
I am of opinion that this patient did not die from the direct effects of the chloroform. The air he was breathing just before he died did not contain more than three or four per cent of vapour of chloroform at the utmost, and he had previously breathed quite as much, both during the same operation and on previous occasions. The patient seemed to be holding his breath at the moment when his heart cessed to beat; and it is whilst holding the breath, and making a straining effort, that patients labouring [208/209] under disease of the heart not unfrequently expire. Mr. Pollock, who was present when the patient died, expressed to me his belief that he died of his heart disease, and not of the chloroform.
After reflecting on this case, I see no reason to regret the course which was pursued. It was the opinion of Mr. Hawkins that the patient could not have borne the operations without the chloroform; consequently, if we had decided not to permit its use any more, in consequence of the alarming syncope which occurred after the operation under its influence on December 4th, 1851, he would probably have died in great suffering from the calculus, instead of having seven or eight months freedom from the complaint. And, on the other hand, if it had been decided to operate without chloroform, it by no means follows that the patient would have been in less danger, judging from what I have observed of the effect of pain on the circulation, as compared with the effect of the chloroform carefully administered, in numerous other cases of disease of the heart.
On May 11th, 1854, a patient died suddenly in St. George's Hospital as she was beginning to inhale chloroform. She was a pale and delicate looking woman, aged thirty-seven, from whose left breast Mr. Cæsar Hawkins was about to remove a mammary glandular tumour. "On entering the operating theatre she appeared nervous. Having been placed on the table on her back, in a half reclining position, the administration of chloroform was commenced. Dr. Snow's inhaler was used. The quantity of chloroform placed in the receiver was a little more than a drachm; and the valve for the admission of air was left wide open. Apparently, from excitement, she did not inhale well, but drew her breath by deep catches, and irregularly. Mr. Potter, noticing this, spoke to her, begging her [209/210] to compose herself, and try to breathe more quietly. The valve was then slightly turned on, in order that she might inhale but a very small quantity of chloroform. The same spasmodic efforts at inspiration still continued; very shortly afterwards, at most not more than a minute and a half from the commencement of the inhalation, Mr. Potter noticed her breathing to suddenly cease, and that she had become deathly pale. The inhaler was at once removed. On placing the finger on the wrist, no pulse could be found. Endeavours to arouse her by dashing the face and chest with water were immediately adopted; but, proving ineffectual, artificial respiration was commenced within a minute of the first symptoms. During the interval, two sighing attempts at inspiration had been observed; but there had been no pulse whatever; the mouth lay a little open, and the countenance was still extremely pale."116 Other attempts at resuscitation were made without effect.
"At the post-mortem examination, on the following day, no very noticeable lesions of the viscera were discovered. There was congestion of the whole venous system, and the blood, in every organ, was of a deep purple colour, and quite fluid. The brain-substance itself was perhaps a little more vascular than usual, and the veins of its meninges were loaded with blood. The heart was small and fat, the right ventricle being especially loaded with adipose material, and its muscular layer much thinned. Under the microscope there was found to be slight, yet decided, fatty degeneration of the muscular structure. Both chambers, but more particularly the right, were distended with blood in which no coagula could be found. The posterior lobes of the lungs were somewhat congested, but not more than the position in which the corpse had lain might account for. There was no disease of the abdominal viscera."117 [210/211]
I made a chemical examination of some blood obtained from the heart and large vessels, and also of portions of the lungs and liver, but I failed to detect any trace of chloroform, although the process I employed is one by which I have very easily detected it in the bodies of small animals killed by it, and also in portions of limbs and tumours removed whilst the patients were under its influence to the usual extent.
It was impossible that this patient could have breathed air strongly charged with vapour. Every one in the operating theatre was a witness that the expiratory valve of the face-piece was not, at any time, more than one-third closed, being two-thirds open. In this way no great effect of any kind can be produced, as very little of the air which the patient breathes passes through the inhaler. Mr. Potter informed me, moreover, that the patient breathed very little even of air, her breathing was so much embarrassed by her frightened condition. He was trying to calm her apprehensions at the moment when she died.
The mental emotion under which the patient was labouring was, no doubt, the cause of the sudden death in this instance, as in that above referred to, which occurred at Mr. Robinson's. The mode of dying, in the present instance, was evidently by cardiac syncope; the same mode of death, in fact, as that which is occasioned by vapour of chloroform, when not sufficiently diluted; and it is only the absolute knowledge, that any small quantity of vapour which this patient inhaled was very largely diluted with air, that enables one to decide, with confidence, that the chloroform was not the cause of death. It may be observed, however, that there was an absence of the convulsive start or spasm which occurred in all those deaths from chloroform, which took place at the beginning of the inhalation, without loss of consciousness having been first induced. [211/212]
The right cavities of the heart were found full of blood in this case, and it is probable that they became so much distended, as the patient was in a state of alarm, and scarcely breathing, that, in the thin and diseased state of the walls of the right ventricle, the action of the heart was arrested. Sudden death not unfrequently takes place during mental emotion, and, in many of the cases, the mode of dying is probably that just mentioned.
Out of the fifty cases of death from chloroform, related above, there are five in which the symptoms at the time of death are not detailed, viz., Cases 6, 7, 21, 24, and 50; in the two first cases it is merely related that the patient suddenly expired, and, in the two last cases, no one was watching the patient at the time when death took place. In considering the remaining cases they may be conveniently divided into groups, according to the period of the inhalation at which the accident occurred. In six of the cases the fatal symptoms came on suddenly, at the beginning of the inhalation, before the patient had been rendered unconscious; in each of these cases there was the most unequivocal evidence of the sudden arrest of the action of the heart. In cases No. 4 and No. 11 there was sudden pallor of the face at the moment when the circulation ceased. In Nos. 14 and 26 the face became livid at the time of the fatal attack, and, in Nos. 45 and 46, the colour of the face is not mentioned. In all these cases there were also symptoms as if of a sudden shock to the system, such as stretching out of the limbs, foaming at the mouth, rolling of the eyes, or a sudden convulsive start. In Case 4, the patient at Boulogne had just complained of a choking feeling, one sign that the vapour she was breathing was not [212/213] well diluted. In Case 11 the fatal symptoms occurred immediately on a full inspiration; and in the other cases also the strength of the vapour was left to accident, and the result leads to the conclusion that it was very great at the moment before the fatal symptoms occurred.
In thirteen cases the inhalation was discontinued on account of the sudden appearance of dangerous symptoms, after consciousness had been apparently suspended. These cases are numbered 9, 15, 17, 20, 27, 30, 33, 35, 37, 40, 41, 44, and 47. In the greater number of these cases the over-action of the chloroform appeared to be exerted simply on the heart, the only dangerous symptoms being referrible to the paralysis of that organ; whilst in some of these cases symptoms of over-narcotism of the brain were conjoined with those connected with the heart. In the case of J. Verrier, No. 9, and in the case at Stockholm, No. 15, the sudden and entire cessation of the pulse was the symptom which first called attention to the danger of the patients, whilst the breathing was still going on. In Case 30 the woman became suddenly insensible and pulseless, after a short period of excitement. In Cases 35 and 40, although the pulse did not absolutely and entirely cease at once, its sudden failure was the first alarming symptom. In Case 20, at the Cavan Infirmary, the breathing and action of the heart ceased at the same moment. In Case 41, at the Middlesex Hospital, at a time when the pulse was full and steady, seventy in the minute, it gave a few rapid and irregular beats, and then ceased, and the breathing, which was free and deep, but not stertorous, ceased at the same time. In Case 15, which occurred at Jamaica, the patient, after a period of excitement, made one stertorous inspiration, when the breathing ceased. There were afterwards a few distant inspirations. The pulse is not mentioned; but it is pretty certain that it must have ceased about the time of [213/214] the stertorous inspiration, or the additional inspirations which took place after the chloroform was withdrawn, would probably have restored the patient; to say nothing of the measures that were resorted to with a view to his resuscitation. Of Case 27, which happened at Melbourne, it is merely related that the patient spluttered at the mouth, and suddenly expired, just after a fresh portion of chloroform had been applied on the handkerchief. The symptom of spluttering at the mouth is recorded as occurring in other cases, just at the moment when the pulse had suddenly ceased.
In Case 44, at the Royal Ophthalmic Hospital, the narcotism of the brain and nervous system proceeded as far as the third degree, which was attended with strong muscular spasms, as not infrequently happens; and an overdose of chloroform appears at this moment to have acted on the heart, for the pulse could not afterwards be felt. In Cases 33, 37, and 47, the narcotism of the brain proceeded as far as the fourth degree, producing stertorous breathing, when the chloroform caused paralysis of the heart, by its direct action on that organ.
There are six cases in which the fatal symptoms came on just after the patient had been rendered insensible, and the inhalation had been discontinued; the operation being about to be commenced. They are numbered 32, 34, 39, 43, 48, and 49. All these cases bear a very close resemblance to each other. In all of them the patient had been made insensible (satisfactorily so as it was thought), when in a few seconds the pulse suddenly stopped, or failed and fluttered just prior to stopping; in Case 32 Dr. Dunsmure thought the time was longer between the discontinuance of inhalation and the cessation of the pulse. The breathing continued a little time after the pulse ceased or failed in all these cases, and there was an absence of the spluttering at [214/215] the mouth, stretching of the limbs, and other spasmodic actions, which occurred in all the six cases where the heart was paralysed at the beginning of the inhalation, before unconsciousness had been induced, and in some of those when the paralysis of the heart took place at a later period of the inhalation, when the patient had been apparently rendered unconscious, but was not yet insensible. In each of the six cases now under consideration, the fatal event was evidently occasioned by the vapour of chloroform, which remained in the lungs at the moment when the inhalation was discontinued. A portion of this vapour becoming absorbed, and added to that already in the blood, had the effect of paralysing the heart, when it circulated through the coronary arteries.
There remain twenty-two cases in which the fatal symptoms came on during the course of the operation. In twenty of these cases the symptoms are described with more or less detail. I made some remarks respecting cases No. 1 and No. 2, in the place where they are related. In case No. 3, as in these cases, the patient appeared not quite insensible, and showed signs of pain during the operation, when "in a moment his pulse, which was full and natural, sank." In case No. 5 the patient was probably dead when the incisions on the finger were commenced; the extreme suddenness of the death, and the absence of bleeding, show that death occurred in the way of syncope. The convulsive movements which just preceded death are worthy of note in connection with the other cases, in which death occurred immediately after the commencement of inhalation. Some remarks were appended to case No. 8. In case No. 10 paralysis of the heart is indicated by the absence of bleeding from the arteries, and the absence of pulse, whilst the breathing still continued for a short time. I made some remarks respecting case No. 12 when it was related. The [215/216] patient seemed to die by embarrassed respiration, but whether that was caused by the action of the chloroform on the brain is doubtful. In case No. 13 the patient died in a moment. In No. 16 the face turned pale, and the pulse and breathing ceased soon after the chloroform was discontinued, showing the effect of the vapour which was present in the lungs at the moment when the inhalation was left off.
In Case 18 the livid countenance and sudden stopping of the pulse prove cardiac syncope. In Case 19 the blood which was gushing out suddenly stopped, and the patient expired. The congested state of the lungs and the blood in the right cavities of the heart prove that the syncope of which he expired was not the ordinary anæmic syncope from hæmorrhage; it was therefore cardiac syncope from the chloroform.
In Case 22 the change of countenance and sudden character of the death are evidences of cardiac syncope. In Case 23 there was sudden cessation of the bleeding and of the pulse; in Case 25 the pulse suddenly ceased. In Case 28 the patient died suddenly, but the pulse was apparently not examined at the time. Some remarks have already been made on Case 29, which happened in the Manchester Infirmary. In Cases 31, 36, and 38 the suddenness of the death showed that it took place by syncope. In the last of these cases the pulse was being examined at the time it ceased. In Case 36 there was no examination of the dead body; but in 31 and 38 the presence of blood in the right cavities of the heart indicates that the kind of syncope was cardiac syncope. Respecting Case 42, some remarks have already been made. The death commenced by deep coma, which embarrassed, and then suspended, the respiration, and cardiac syncope quickly followed. The chloroform was administered by a method which precluded the medical attendant from observing properly the most important symptoms. [216/217]
The accompanying table [pp. 218-21] of the fatal cases of the inhalation of chloroform contains such short particulars respecting them as seemed capable of being tabulated, and it may assist the reader in retaining a more connected recollection of the facts previously related more in detail.
In all the cases in which the symptoms which occurred at the time of death are reported, there is every reason to conclude, as shown above, that death took place by cardiac syncope, or arrest of the action of the heart. In forty of these cases the symptoms of danger appeared to arise entirely from cardiac syncope, and were not complicated by the over-action of the chloroform on the brain. It was only in four cases that the breathing appeared to be embarrassed and arrested by the effect of the chloroform on the brain and medulla oblongata, at the time when the action of the heart was arrested by it; and only in one of these cases (No. 42) that the breathing was distinctly arrested by the effect of the chloroform, a few seconds before that agent also arrested the action of the heart.
It was previously shown that chloroform vapour has the effect of suddenly arresting the action of the heart when it is mixed with the respired air to the extent of eight or ten per cent, or upwards; and we must therefore conclude that, in the fatal cases of its inhalation, the air the patients were breathing just before the accidents occurred contained this amount of vapour. There was no means adopted, so far as is reported, to regulate the proportion of vapour in the inspired air, in any case in which an accident happened; and there was the liability in every case that ten per cent or more of vapour might be present in the air the patient breathed; and in no case did death occur in the manner that it occurs when the vapour of chloroform does not exceed five per cent of the inspired air. [217/218]
(click on images to view expanded version)

[218/219]

[219/220]

[220/221]

[221/222]
There is in a great number of the cases an evident connection between the accident and the probable strength of the mixture of vapour and air. In six cases the accident occurred just after the commencement of the inhalation; in two of the cases, Nos. 27 and 37, the fatal symptoms occurred just after fresh chloroform had been applied on the handkerchief and sponge; and in several cases, in which the circulation was suddenly arrested just after the patient had been rendered insensible, the insensibility had been induced so quickly as to prove that the vapour must have been inhaled in a very insufficient state of dilution.
Dr. Patrick Black has made an objection to the fact of the patients having died of paralysis, or over-narcotism of the heart, in the accidents from chloroform.118 He says that paralysis of the heart would be death by syncope, but that the symptoms before death, and the conditions of the organs met with afterwards, are not in accordance with such a view of the case. In order to show that both the symptoms and the after death appearances, in the fatal cases of inhalation of chloroform, are consistent with paralysis of the heart, it is necessary to point out the difference between ordinary syncope and cardiac syncope. One of the best examples of ordinary, or what may be called anemic syncope, is that which occurs in a common blood-letting, whilst the patient is in the sitting posture. When the bloodvessels, especially the veins, which at all times contain the greater part of the blood in the body, do not accommodate themselves fast enough to the diminished quantity of blood, the right cavities of the heart are supplied with less and less of the circulating fluid; and in a [222/223] little time are not supplied at all, when the heart ceases to beat, in accordance with the observation of Haller, that it does not pulsate when it is not supplied with blood. The moment the heart ceases to supply blood to the brain there are loss of consciousness and stoppage of respiration; but on the patient being placed in the horizontal position the blood flows readily into the right cavities of the heart from the great veins of the abdomen and lower extremities; the heart immediately recommences its contractions; the brain is again supplied with blood, and respiration and consciousness return. 119
The blood may remain in the ordinary quantity; but if the bloodvessels do not keep up their usual support, and exert a sufficient pressure on their contents, the same kind of syncope will occur as that from blood-letting. The late Sir George Lefevre related the case of a lady who fainted whenever she left her bed, and assumed the upright posture; no cause could be found for this until it was ascertained that she suffered from varicose veins of the legs: bandages to these extremities prevented the fainting. It is obvious that in this case the mechanism of the syncope was the same as that in blood-letting; the distension of the varicose veins under the weight of the superincumbent blood had the same effect in preventing the supply to the right cavities of the heart, as if the blood had been entirely removed. The faintness which often occurs on first rising, when a person has long kept the recumbent posture from [223/224] any local cause, is probably of the same kind; the veins not having had to support the weight of the usual column of blood for some days or weeks, lose their tone we may presume, and yield when they are all at once subjected to the weight of a column of blood extending from the lower extremities to the heart, so that this organ ceases to be properly supplied with the circulating fluid.
In cardiac syncope, on the other hand, the cavities of the heart, or at all events the right cavities of this organ, are always full, whether the syncope depend on paralysis of the heart by a narcotic, or inherent weakness of its structure, or on its being overpowered by the quantity of blood with which it is distended. After death from this kind of syncope, if the blood have not been displaced by artificial respiration or other causes, the right cavities of the heart and the adjoining great veins will be found filled with blood, and the lungs will in many cases be more or less congested. The appearances in short will be very much the same as in asphyxia by privation of air, which ends in a kind of cardiac syncope, the stoppage of the heart being partly due to over-distension of its right cavities, and partly to loss of power in its structure, from the want of a supply of oxygenated blood through the coronary arteries. In death by anæmic syncope, on the contrary, all the cavities of the heart are found empty, or nearly so, and the same is frequently the case with the adjoining great veins, whilst the lungs are usually pale.
The syncope occasioned by some kinds of mental emotion is of the ordinary or anæmic kind, and consequently the condition of the brain must act first on the bloodvessels, and not directly on the heart. Certain persons are liable to faint on witnessing a surgical operation. Now if the mental emotion of these persons acted directly on the heart, whilst the rest of the vascular system was unaffected, the distribu-[224/225]tion of the blood would be nearly the same as in asphyxia, where the circulation is first impeded in the lungs, and is ultimately arrested by loss of power in the heart. If the action of the heart were weakened, or stopped, in the first instance, by the kind of emotion under consideration, the arteries would be emptied by their contractility and elasticity, and the blood would accumulate in the right cavities of the heart and the great veins leading to them. In a medical student fresh from the country, who is by no means deficient in blood, the jugulars would become distended and the face livid, and the recumbent posture would probably do but little towards removing the symptoms. The phenomena which are witnessed, however, indicate a very different condition of the vascular system. The person about to faint from the cause indicated, frequently becomes pale before he feels anything wrong; and when requested to retire and sit down, often says that there is nothing the matter with him. In a short time he faints, and falls, if no one catches hold of him; but the moment he is in the recumbent posture he recovers. In such a case as this, the effect of the mental emotion must be first exerted on the veins, or the veins and capillaries, through the nerves which supply these vessels; they allow themselves to become distended, and the heart ceases to act for want of its supply of blood, as in syncope from bloodletting, and anæmic syncope from any cause.
Several authors have attributed the empty state of the heart met with after death, in certain cases of fatal syncope, to want of power in the left ventricle to supply the right cavities of the heart; but this is to argue as if the blood passed out of the body after leaving the right ventricle, and the left ventricle had to supply a newly formed fluid. The effects of want of power in the left ventricle are the same as those of an obstruction at the origin of the aorta; the lungs become congested, and the right cavities of the heart more [225/226] or less distended, from the blood not being able to pass readily through the lungs. Patients who die of heart disease die with the cavities of that organ full. Some patients, indeed, with fatty disease of the heart, die suddenly of anæmic syncope, and the heart is found empty; but in these cases it is evident that death is not occasioned by the disease of the heart, but by some condition of the bloodvessels which accompanies it.
Chevalier was, I believe, the first to draw marked attention to cases of sudden death arising from an empty state of the heart, in a paper in the first volume of the >em>Transactions of the Royal Medical and Chirurgical Society; and he rightly attributed the emptiness of the heart to a loss of power in the bloodvessels. His words are as follow:--
"The disease I have now described may, perhaps, be termed
The word asphyxia has become so closely connected by physiologists with death by privation of air, where the symptoms and appearances are the reverse of those in Chevalier's case, that it is necessary to discard his name of the disease which he describes, although it is etymologically correct. His cases come under the definition of what is now universally called syncope, and what I have called anæmic to distinguish it from cardiac syncope.
Chevalier speaks of a want of power in the vessels to propel the blood, and as it is not now believed that the vessels take any active share in the propulsion of the blood, this may be the reason why the views of this author have received less attention than they deserve; but it is very ob-[226/227]vious that a want of tone in the vessels, or any great diminution of that power which enables them to support and compress the blood, is an adequate cause why the blood should be unable to reach the right side of the heart. In the case of varicose veins, previously mentioned, it was physically apparent that the cause of the syncope lay in the vessels. Disease of the arteries is well known to be usually associated with degeneration of the heart; the veins are also large and distensible in old people, who furnish the greater number of those who are liable to anæmic syncope; but the pathology of the veins, as regards both their functions and structure, is not yet sufficiently known.
Persons with disease of the heart, who die suddenly in a fit of anger, probably die always with the heart distended; that is, of cardiac syncope. Dr. Joseph Ridge, however, in his able and interesting remarks on the disease and death of John Hunter,120 states his belief that that celebrated man, who had been long subject to attacks of angina pectoris, died at last of syncope, with an empty heart. He died, as is well known, during a fit of anger, and the coronary arteries were found ossified. It is not said that the heart was empty, but that it was small, and that there were no coagula in any of its cavities. It is probable that there was not much blood in its cavities, at the time of the post mortem examination, but the body of Hunter was conveyed in a sedan-chair, from St. George's Hospital to Leicester Square, a little more than an hour after his death, so that the fluid blood would gravitate downwards. It is related that the stomach and intestines were unusually loaded with blood, and that those parts which were in a depending position, as in the bottom of the pelvis and upon the loins, were congested in a greater degree than the others; and that "this evidently arose from the fluid state of the blood." [227/228]
In syncope from muscular exertion, the cavities of the heart are distended, and its walls have occasionally been ruptured, both from violent exercise and fits of anger.
Fear probably occasions each kind of syncope in different cases. In some cases, the right cavities of the heart become distended owing to impeded respiration, and possibly to a diminution of power in the heart itself. More frequently, the syncope appears to be of the ordinary or anæmic kind, the effect of the mental condition acting first on the more distant parts of the circulation. The pallor caused by fright is proverbial.
Pain is also capable of causing both kinds of syncope. I have alluded to cases in which the patients strained and held their breath till the pulse became intermittent, and the action of the heart was temporarily suspended by the arrested breathing; on the other hand, patients often become pale, if they are undergoing any slight operation when seated, and syncope of the anæmic kind occurs, without any previous disturbance of the respiration, but passes off as soon as they are placed in the horizontal posture. I have seen an apparently strong man faint in this manner, during the removal of a tumour from the back not larger than a nut, and where only a few drops of blood were lost. Chloroform was not employed.
Many writers have supposed that the deaths from chloroform have arisen from some peculiarity in the patient; and when any notable change of structure has been met with after death in any of the vital organs, this has been thought to afford a sufficient explanation of the event; whilst in the cases in which the organs were in a healthy state, surprise has been expressed at the occurrence. In looking over the account of the cases in which the inhalation of chloroform [228/229] has been fatal, there is reason to conclude, however, that the subjects of them were, as regards health and strength, quite equal to the average of the multitude who have inhaled this agent without ill effects. In fifteen out of the fifty cases above related, there was no examination of the body after death. In one of these fifteen cases, the patient was in a state of debility, and had hectic fever, apparently from the disease of the ankle-joint, for he had no cough; in another of these cases, the patient was reduced to a state of great debility from cancerous disease of the uterus. In fourteen out of the thirty-five cases, in which an examination of the dead body took place, all the chief organs were found to be healthy, if we except the local congestions of blood connected with the mode of dying, and a flabby state of the heart in a few of the cases, which probably depended on its being full of blood at the time of death, or its not being in a state of post mortem rigidity, at the time it was examined.
In one case, No. 25, the only morbid appearances were adhesions of the pleura of small extent; and in No. 47, the only disease was fatty liver. In Case 17, there were signs of chronic disease of the membranes of the brain; and in two cases, Nos. 16 and 22, there was emphysema of the lungs. In the remaining sixteen cases, there was some alteration of the heart, accompanied in a few instances by disease of other organs. In Cases 23 and 32, there was fat on the surface of the heart, but the structure was not degenerated. In Case 43, the right ventricle was thinned, but not fatty. In Case 44, there were slight deposits on the mitral valve, the heart being otherwise healthy. In Case 50, there were deposits of lymph on the mitral valve and also on the surface of the heart, which was somewhat enlarged. In Case 8, the heart is merely stated to be large; and in Case 27, hypertrophied. In Case 3, the heart was enlarged, pale, and soft, and the lungs were tuberculous. In Case 15, [229/230] there was said to be some amount of disease of the aortic valves, and some amount of fatty degeneration of the heart. In Case 37, incipient fatty degeneration was present; and in Case 40, that of a youth of eighteen, the heart was slightly enlarged, with some amount of fatty degeneration. In Case 46, the right ventricle was thinned and slightly fatty. There remain three Cases, Nos. 30, 33, and 42, in which the fatty degeneration was more decided; and one case, No. 41, in which it is spoken of as being present in an extreme degree. This was in a man, aged sixty-five, the oldest person included amongst those who died from chloroform.
When we consider how common is fatty degeneration of the heart, especially amongst old persons and those for a long time confined to bed, it is very probable that this affection has been proportionally as frequent, amongst the patients who have inhaled chloroform without ill effects, as in the fatal cases of its inhalation.
There are nine of the fatal cases in which the age of the patient is not stated. In the other forty-one cases, the ages, when grouped in decennial periods, are shown in the following table, the last column of which shows the proportion which the deaths bear at each period to the number living at that period, out of a thousand persons of all ages in England and Wales.

The nine persons whose ages are not given were all adults; one is spoken of as a young man, and another as a young woman, and the rest are mentioned in such a manner that it is certain they were not old people. It follows, therefore, that so far as is known, there has been a complete immunity from death by chloroform at both extremes of life. I have already given my reasons for rejecting Dr. Aschendorf's case of an infant, and also the case of a gentleman, aged seventy-three, who died whilst inhaling chloroform. The youngest patient who died from chloroform was seven or eight years of age, and the oldest sixty-five, being the only death above sixty. The above table of the ages shows that the number of deaths, in proportion to the number living, increased rapidly after the age of twenty-five, and decreased rapidly after the age of forty-five. The small number of deaths between fifteen and twenty-five may be partly due to the circumstance that surgical operations are but seldom required at this period of life; but the decrease after the age of forty-five cannot be explained in this way; for persons become more liable to require surgical operations as they advance in years. Operations are often performed in infancy and old age, periods at which deaths from chloroform have not been recorded. The greatest proportion of deaths having occurred from thirty-five to forty-five, when the system is often more robust than at any other period, it cannot be supposed that an inability to bear the usual dose of chloroform, when carefully administered, is the ordinary cause of death from this agent.
Idiosyncrasy. The accidents from chloroform have frequently been attributed to idiosyncrasy in the patient. This, it may be observed, is not to give an explanation of them, but merely to state that they depend on something we do not understand; that something, however, being in the person to whom the accident happens. This view receives [231/232] apparent support from the supposition that the chloroform has been inhaled in exactly the same manner in the fatal cases as in other instances; but this apparent support fails when it is pointed out that the supposed same manner is only an equally uncertain manner. The different effects that have been produced on the same patient at different times, and the great number of instances in which medical men have failed to make the patient insensible, show that most of the usual modes of exhibiting chloroform are extremely uncertain.
What most completely meets the question of idiosyncrasy, however, is the circumstance that in no fewer than eleven out of the fifty recorded cases of death from chloroform, the patient had previously inhaled this medicine without ill effects. In two other cases also, previous attempts had been made to make the patient insensible without success, on the day on which the accident occurred. In the above table of the fatal cases, those are indicated in which previous inhalations had taken place. In twenty-nine cases, I have concluded that the patient had not previously inhaled, for the medical man, having given an account of the state of his patient, and his reasons for administering the chloroform, would certainly have mentioned such a material fact as a previous inhalation if it had occurred. There are ten cases of which only a meagre account is given, and where a previous administration of chloroform may possibly have taken place without being mentioned; but if only eleven, out of the fifty patients, who died from chloroform, had inhaled it previously without ill effects, it is very clear that the fact of having inhaled it with a favourable result, gives no immunity from the possibility of accident. It would be impossible to say what proportion of the patients who have inhaled chloroform have inhaled it more than once, but it is not probable that they amount to more than 22 per cent, if so many. [232/233]
Alleged Impurity of the Chloroform. At one time accidents from chloroform were loosely attributed to impurity in the medicine, but this was only a guess, and is opposed to the facts. No case of accident has been traced to this cause, and in nearly all the cases of which the details are given, it is distinctly recorded, either that the chloroform was examined and found to be of good quality, or else that chloroform out of the same bottle had been used in other cases without ill effects. I have not thought it necessary to state this in quoting the individual cases.
Apparatus employed. Accidents were at one time, and in one quarter, attributed to the use of inhalers; and it is curious that this allegation was made at a time when no death from chloroform had yet occurred in any cases in which an inhaler was used, except one in America, and one in France, the accounts of which had not reached this country. It is possible that death might be occasioned by want of air from the use of a faulty inhaler, and a case will be mentioned in which this apparently occurred in the administration of sulphuric ether, but there is no recorded case of accident from chloroform in which death was occasioned in this way. In the cases of death previously recorded, a handkerchief, a piece of folded lint, hollow sponge, or some such simple contrivance, was used in thirty-four instances; in twelve cases, an inhaler of some kind or other was used; and in four cases, it is uncertain what were the means employed.
Alleged Exclusion of Air. The assertion has often been made that death might be caused by the vapour of chloroform excluding the air, and so causing asphyxia; but it has already been pointed out in this work that the physical properties of chloroform do not allow it to yield a quantity of vapour which would have that effect, and in much smaller quantity than this the vapour kills by a quicker way than [233/234] asphyxia, I believe that the only elastic fluids which can cause death simply by excluding the atmospheric air are nitrogen and hydrogen.
Alleged Closure of the Glottis. At the trial which took place in Paris respecting the death of a porcelain dealer previously mentioned, M. Devergie gave evidence, and after saying that chloroform might cause death as a poison, if given in undue proportion, he added: "Also it closes the glottis, and offers an obstacle to respiration. Employed by M. Demarquay on himself, in very small doses, closure of the glottis was occasioned. It was possible that Le Sieur Breton had experienced that accident, and in that case the most able surgeon could not prevent death."
I have not met with M. Demarquay's account of his experiment, but I am happy to know that he did not die of the closure of the glottis. It may fairly be denied that a person could commit suicide in this manner if he wished, for he would either have to give up the attempt, or receive the vapour into his lungs, and experience its specific effects. When animals are placed in mixtures of vapour and air, they always breathe them, whatever the strength; and if the vapour amounts to eight or ten per cent, they die much more quickly than they would of mere closure of the glottis. Vapour of chloroform, when not largely diluted with air, is apt to cause cough and closure of the glottis, as soon as a little of it reaches the lungs; but this, so far from being a source of danger, is, as a general rule, a safeguard, by its preventing the patient from readily breathing air which is highly charged with vapour.
In commenting on the fatal case No. 12, which occurred in St. Thomas's Hospital, I have suggested that the accident might have happened from liquid chloroform being dropped into the throat; but liquid chloroform is very different from the vapour; it causes a lasting irritation if applied to a [234/235] mucous membrane; when used for toothache, it often blisters the gums. The irritation caused by the vapour, on the contrary, is only momentary, and its local action ceases directly it ceases to be inhaled; for what is left in the air passages is immediately absorbed or expelled with the expired air. The glottis is not a vital organ of itself. Its closure only causes death by preventing the access of air to the lungs. The glottis does not remain permanently closed, I believe, from the contact of any elastic fluid, however irritating;121 but it does from the contact of a liquid, and persons who die by drowning, die with the glottis closed, for they do not fill their lungs with water. Therefore, if the vapour of chloroform did cause persistent closure of the glottis, and if a person were to hold it by force to the patient, the death it would occasion would be precisely like that in drowning. Death by asphyxia is a comparatively slow one. I find that when the access of air to the lungs is entirely cut off, death does not take place in less than three minutes and a half in guinea pigs, and four minutes in cats. In dogs, the process of asphyxia is still slower. Mr. Erichsen states, that on taking the average of nearly twenty experiments, the contractions of the ventricles continued for nine minutes and a quarter after the trachea had been closed, and that the pulsations of the femoral artery also were perceptible for an average period of seven minutes and a half. The process of drowning in the human subject is well known to occupy some minutes; and even if the pungency of the vapour of chloroform should entirely prevent the patient from breathing, and the medical man could overlook the fact that breathing was not going on, it cannot be supposed that he would use the force, and have the perseverance to [235/236] cause his patient to die slowly by asphyxia. If any patient, therefore, has died from closure of the glottis, it must have been one in whom there was a great tendency to sudden death from any slight interruption to respiration. I do not know the particulars of the case respecting which M. Devergie was giving his evidence, but in those fatal cases previously related, in which the symptoms are sufficiently described, it is not probable that death took place in any instance from closure of the glottis. In the sudden death at St. George's Hospital (page 209), it is possible that the slight pungency of the vapour might assist the fear under which the patient was labouring in impeding the breathing, and thus add to the distension of the right cavities of the heart, under which the patient apparently died.
In 1855, two years after M. Devergie had given the above opinion, Dr. Black, of St. Bartholomew's Hospital, who has had great experience in the administration of chloroform, advanced a similar theory in the pamphlet previously alluded to. He did not, however, confine the effects of the supposed closure of the glottis to possibly causing a death here and there, as M. Devergie had done, but he attributed all the accidents which had happened to this cause, and not to the effects of chloroform in the system. He says that "the chloroform has not been even inhaled: its pungency was felt at the glottis, and its inspiration was immediately arrested. The patient would have removed the apparatus, but in this he was restrained. The struggle forthwith commenced, but up to the moment of his death, not a single inspiration took place." These remarks were not applied to a single case, but generally to the accidents from chloroform. Dr. Black says: "Any concentration of the vapour of chloroform which can be breathed is safe; any condition of dilution which forces the patient to cough or hold his breath is dangerous, and if persevered in for even half a minute, [236/237] may be fatal. . . . We have only to attend to the breathing; we may disregard all considerations affecting the relative proportion of the chloroform in the air which is breathed; . . . if the patient breathes easily he is in safety, whatever be the amount of chloroform which is passing into the lungs."
In Experiment 28, previously related, where the respiration was kept up by a tube in the trachea, there could be no error in respect to the vapour of chloroform entering the lungs, when a bladder of air charged with ten per cent of that vapour was substituted for the bladder of simple air; and the immediate paralysis of the heart was evident. An examination of the fatal cases, of which the particulars have been recorded, shows that death did not occur in the manner Dr. Black suggests. In the majority of the cases, the patients were rendered quite insensible by the chloroform, and the operation had either been commenced, or was on the point of commencing, when the fatal symptoms set in. In several other cases, the patients were partially under the influence of the vapour before the symptoms of danger commenced; and in the six cases where death occurred at the beginning of the inhalation, without loss of consciousness having been induced, the patients were not restrained in any way, and it was observed that they did breathe the chloroform; three of them were speaking up to the moment when the pulse stopped, and one took a full inspiration the moment before the fatal symptoms set in. It is only in eighteen of the fatal cases that there is any reason to suppose that the patient required to be held, and then only from mental excitement or muscular spasm, arising from the physiological effects of the absorbed chloroform. It is hardly possible that the struggles of a conscious patient from inability to breathe, would be mistaken for excitement or spasm caused by chloroform. [237/238]
In a case, No. 34, which occurred at St. Bartholomew's Hospital whilst Dr. Black was present, and long before his pamphlet was written, the patient inhaled for five minutes, and sank off into a state of complete insensibility without alarming symptoms. The inhalation was discontinued, the patient moved into a proper position, and the operation just about to be commenced, when Dr. Black found the pulse to become extremely feeble and fluttering. Surely this patient breathed the chloroform, and died without any spasm of the glottis. In Case 48, so minutely related by Mr. Paget, the boy made one long inspiration, and became suddenly insensible. In a few seconds, the pulse suddenly failed, and then ceased to be perceptible, but the breathing continued for at least a minute afterwards. There was certainly no closure of the glottis in this instance.
Alleged Exhaustion from Struggling. In cases where the patients have struggled violently whilst getting under the influence of chloroform, the accidents have been attributed to a supposed exhaustion caused by the struggling.122 This opinion is, however, contrary to experience; for the patients who struggle violently are precisely those who bear chloroform the best, provided they do not breathe it in an insufficient state of dilution. They are generally cheerful and exhilarated by it, and are less liable to be depressed by its prolonged use, than those who come quietly under its influence. Although the patients who struggle bear the chloroform well, when it is carefully and judiciously administered, it is not improbable that the struggling has been now and then an indirect cause of accident. The muscular spasm and rigidity do not occur till about three-quarters as much chloroform has been absorbed as can be present in the system with safety; and, as the patients often hold their breath whilst struggling, and take deep inspirations sud-[238/239]denly and at long intervals, the greatest care is required that the vapour be administered in a very diluted state. In Cases 9, 44, and 47, the fatal symptoms came on whilst the patients were struggling; and in some other cases, the sudden failure of pulse occurred just after the struggling had ceased, rendering it probable that the patient inhaled too much of the vapour whilst struggling, or just as the spasmodic condition of the muscles was subsiding.
The circumstances just mentioned, are probably the cause why so many of the fatal cases occurred at that period of life when the body is most robust. Very nearly two-thirds (twenty-seven out of forty-one), of those cases in which the ages are recorded, occurred in persons of twenty years and under forty-five years of age, although the proportion of persons living at this period of life, in England and Wales, is only a little more than one-third of the entire population. The majority of the accidents from chloroform occurred also in the stronger sex, in which muscular rigidity and spasm are most frequent:--twenty-nine of the fatal cases happened to males, and only twenty-one to females. According to my experience, the females who inhale chloroform for surgical operations are nearly twice as numerous as the males; and although this may not be the proportion in every one's practice, it is probable that females inhale this agent quite as frequently as the other sex, in every part of the world.
Sitting Posture. In some of the early cases of death from chloroform, the patients were inhaling it in the sitting posture, and it was surmised that this circumstance was the cause of death.123 An examination of the account of the fatal cases, however, does not bear out this supposition. In thirty-one instances the patients were lying, in nine instances sitting, and there are ten cases in which the position [239/240] is not mentioned, and where from the nature of the operation it may have been either one or the other. In fully one-fourth of the cases of which I have kept notes of the administration of chloroform, the patients were seated in an easy chair; and as in forty fatal cases in which the position is known, only nine, or less than one-fourth, were seated, it does not appear that the position of the patient has had any share either in causing or preventing accidents.
Supposed Effect of the Surgeon's Knife on the Pulse. Mr. Bickersteth alluded to a peculiar circumstance,124 which he thought would account for several of the deaths attributed to chloroform. He relates three instances in which the pulse suddenly ceased on the first incision by the surgeon, and commenced again in a few seconds, the breathing going on naturally all the time. All the three cases were amputation of the thigh, and occurred in the latter part of 1851. Mr. Bickersteth did not observe the circumstance again during the two following years, and I have never observed it, although I have very often examined the pulse at the moment when the operation began, especially after reading Mr. Bickersteth's remarks. He supposes that the action of the heart was arrested by the shock of the incision, notwithstanding the patient was insensible. I should attribute the temporary stoppage of the pulse in these instances to the direct influence of the chloroform on the heart. The moment when the operation is commenced, is usually a few seconds after the inhalation has been discontinued, and when the effect of the chloroform is at its height. A portion of that which was left in the lungs having been absorbed, in addition to that which was previously in the system. And if the vapour inhaled just at last was not sufficiently diluted, it might paralyse the heart, but not so completely as to prevent the natural respiration from restor-[240/241]ing its action, in those cases where respiration continues. I found in experiments on animals that, when the action of the heart has been suspended by the effect of chloroform, it can very often be restored by artificial respiration instantly applied; and it is extremely probable that an accident of this kind not unfrequently occurs during the administration of chloroform, and is remedied by the breathing, without being noticed. The pulse recovered itself, in the cases mentioned by Mr. Bickersteth, just as it does in animals after the heart has been nearly overpowered by chloroform. In the first case, the pulse remained imperceptible for a period of four or five seconds, the countenance at the same time becoming deadly pale. As it returned, it was at first very feeble, but in a few seconds, it regained its usual strength. In the second case, Dr. Simpson administered the chloroform, and after the operation remarked that the pulse had stopped suddenly just as the knife was piercing the thigh, and had recovered itself with a flutter almost immediately.
Mr. Bickersteth's reason for attributing the stoppage of the pulse to the effect of the knife, rather than the chloroform, was that he had arrived at the conclusion from some experiments which he performed on animals, that the action of the heart cannot be arrested by chloroform, until the breathing has been first suspended. One of Mr. Bickersteth's experiments (No. 5, on a half-grown cat) exactly resembles the experiment (No. 28 in this work) on a rabbit, which I had published upwards of a year before Mr. Bickersteth's paper appeared, with the exception that in my experiment the artificial respiration was performed with air containing ten per cent of vapour, and in Mr. Bickersteth's the vapour was an unknown quantity. In both experiments, the heart of the animal was exposed. In that which I performed, three or four inflations of the lungs almost paralyzed the heart; and nine or ten inflations, which did [241/242] not occupy half a minute, had the effect of paralyzing that organ irrecoverably. In Mr. Bickersteth's experiment, the effect of the artificial respiration was as follows:--"After continuing it for seven minutes, the diaphragm, hitherto unaffected, began to move very irregularly and imperfectly; then its movements became slow and hardly perceptible; and, at the expiration of eleven minutes, they had ceased altogether. During all this time the heart's action remained strong and regular, but now it got weaker and more rapid, and, in four minutes from the time the diaphragm had ceased acting, had become so feeble (still quite regular) that I feared every moment it would stop." Mr. Bickersteth says he performed artificial respiration with air saturated with chloroform; but saturated or not, the vapour certainly did not exceed six per cent, and most likely was only between four and five, if the artificial resembled the natural respiration in quantity and frequency. The vapour which can be breathed for seven minutes without causing serious symptoms, and for eleven minutes without arresting the breathing, is of course incapable of stopping the action of the heart by its direct effect. It is scarcely so strong as that which one administers every day to patients with impunity. The vapour which is so diluted as to require to be added by small increments during one hundred and fifty inspirations, before the brain is even narcotized, cannot act directly on the heart, an organ which can bear a much larger amount of chloroform. Mr. Bickersteth fell into the error into which the Committee of the Society of Emulation of Paris afterwards fell, and argued from the rule to the exception. What he witnessed was the mode of death which would occur, if vapour of chloroform of the strength which can be safely inhaled, were deliberately continued till the death of the patient. But an accident from chloroform is an exception, and the mode of dying is as much an exception [243/244] as the death itself, if the inquiry is extended to what this agent is capable of doing, instead of confining it to what one endeavours to effect with it in the human subject alone.
So many of the deaths during the inhalation of chloroform have occurred before the operation had commenced, or after it had proceeded some way, that Mr. Bickersteth's explanation would not apply to a great number, even if it were correct; and when it is remembered that the operation is always commenced when the effect of the chloroform is expected to be at its height, the number of cases of cardiac syncope which have happened at the beginning of the operation is not greater than might be expected as the result of the effect of chloroform.
Sudden Death from other Causes. It has been more than once suggested that the deaths which have occurred, during the inhalation of chloroform, are of the same nature as the sudden deaths which have often occurred about the time of surgical operations, apparently without any adequate cause; and that in fact the accident and the chloroform may be a mere coincidence, and not connected as cause and effect. It has been already shown that the Commission of the Academy of Medicine of Paris made this suggestion in treating of the case of Madlle. Stock, and Dr. Simpson has more than once made a similar remark. On one occasion,125 he remarked, in speaking of chloroform:--"The first surgical cases in which it was used were operated upon in the Royal Infirmary here, on the 15th of November, 1847. Two days previously, an operation took place in the Infirmary, at which I could not be present, to test the power of chloroform; and so far fortunately so; for the man was operated upon for hernia, without any anæsthetic, and suddenly died after the first incision was made through the skin, and with the operation uncompleted." I should say, so far unfor-[243/244]tunately so, for whatever the cause of the man's death, that cause could hardly have been present if the patient had been made insensible by chloroform; and so his life would in all probability have been saved. If he died either from fear or from pain, the chloroform would have prevented his death, by removing and preventing these causes; and if his death arose from simple exhaustion, it must be remembered that chloroform is a stimulant, during the first part of its administration, and, as a general rule, so long as it is actually in the system. Even Mr. Bickersteth, who thinks that the knife of the surgeon may have a direct influence on the heart when the patient is quite insensible, expresses his conviction that such an occurrence is far less likely to happen under the influence of chloroform than in the waking state.
I have omitted from the list of deaths by chloroform two cases which are usually attributed to that agent, namely, the case of Mr. Robinson's patient, and the one at St. George's Hospital, and have attributed them to fear; and I also rejected the case of the infant on which Dr. Aschendorf operated, for the reasons I stated; and it is quite possible that amongst the fifty cases I have retained, there may be one or two in which the death was not caused by chloroform, especially as the details of some of the cases are very meagre; but when all the circumstances of the cases are examined, and especially when the mode of death is compared to that which chloroform can be made to produce in animals, it cannot be supposed that the fatal event was a mere coincidence in the whole fifty cases, or in any great number of them.
There are numerous instances recorded of sudden death during surgical operations, or just before intended ones, without any evident cause, except fear or pain, before the use of narcotic vapours was known; and some even since, in cases in which it was not thought worth while to use [244/245] them. After the passage quoted above, Dr. Simpson continues:--"I know of another case in Edinburgh, where death instantaneously followed the use of an abscess-lancet without chloroform,--the practitioner, in fact, deeming the case too slight to require any anæsthetic." Such events have, no doubt, often happened without being recorded; and it is extremely likely that the deaths of this kind which chloroform has prevented are quite as numerous as those it has occasioned by its own effects, but the medical profession will very properly not be satisfied with a result of this kind, if more can be done; and the endeavour of the practitioner of course is, whilst saving life as well as preventing pain by the use of this agent, to avoid as far as possible having any accident from its use.
Falling back of the Tongue. It has been alleged that the falling back of the tongue into the throat, under the deep influence of chloroform, might be the cause of death by suffocation; but this appears to be an error; for the muscles of the larynx and neighbouring parts preserve their action as long as the diagraphm [sic], and contract consentaneously with it. When the breathing has ceased, the tongue is indeed liable to fall backwards, if the person in a state of suspended animation is lying on the back, and this circumstance requires to be attended to in performing artificial respiration.
A few years ago, I examined the viscera of the chest, and kept notes of the appearances, in thirty-seven animals killed by chloroform. They consisted of two dogs, twenty-two cats, one kitten, three rabbits, three guineapigs, two mice, two larks, and two chaffinches. Many of the animals were opened immediately after death, and the rest within a day or two. The lungs were not much congested in any in-[245/246]stance. In seven of the animals, they were slightly congested; but in the remaining thirty, they were not congested. They were generally of a red colour, but in a few of the cats they were quite pale. I ascertained the specific gravity of the lungs of two of the cats, in which they presented the amount of vascularity I have most usually met with. The specific gravity was 0.605 in one instance, and 0.798 in the other. As many of the animals died in a way resembling asphyxia, the respiration ceasing before the circulation, it might at first be supposed that we should meet with the same congestion of the lungs; but by the time that the respiration is altogether suspended by the action of chloroform, that agent has begun already to influence the heart, which does not inject the blood into the lungs with the same force as when the respiration is mechanically prevented, whilst it is in full vigour. Besides, in the gaspings which so often take place when the heart is ceasing to act, the animal inhaling chloroform draws air freely into the lungs, whilst the asphyxiated animal is prevented from doing so.
As regards the condition of the heart, it was found in the two chaffinches that the auricles were filled with blood, whilst the ventricles were empty. The condition of the heart in the larks is not mentioned, but in all the thirty-three quadrupeds, the right auricle and ventricle were filled with blood. In ten of them, these cavities were much distended; and in some of these instances, the coronary vessels on the surface of the heart were distended also. The left cavities of the heart never contained more than a small quantity of blood, not exceeding a quarter of what they would hold.
The head was examined in only ten of the animals. The substance of the brain was found to be of the natural vascularity, and the sinuses were not very much distended, except in two instances. [246/247]
With respect to the state of the blood, it may be mentioned, that in every instance in which the chest was opened within an hour after death, the blood which flowed from the cut vessels coagulated immediately and firmly. In eighteen of the animals in which the blood was examined in the heart or large vessels, a day or two after death, it was found to be well coagulated in ten, loosely coagulated in seven instances, and quite fluid in one instance. I have not met with air in the bloodvessels, either in the above thirty-seven examinations, or in any of the numerous other animals that I have opened, after they have been killed by chloroform. The appearances I have met with in animals killed by this agent have usually been such as I have described in the above thirty-seven instances; but I, long since ceased, as a general rule, to make careful notes of the appearances, as I did not meet with anything new.
In the fatal cases of inhalation of chloroform previously quoted, the lungs are related to have been congested more frequently, and to a greater extent, than I have met with in animals. But there is no standard of what should be called congestion; and probably many of the medical men who made the examinations were speaking by comparison with cases where persons die after illness, in a state of inanition. In the human subject, the right cavities of the heart, although generally full of blood, were found empty in several cases; but as I previously stated, it is almost certain that they were emptied after death, either by the artificial respiration which was employed, or in some other way.
The blood remained fluid in eighteen out of twenty-five cases of fatal accident from chloroform, in which an examination of the body was made and the condition of the blood recorded; whereas it was only quite fluid in one instance out of eighteen of the animals which were killed by chloroform, and not opened till a day or two afterwards. [247/248]
The fact of the blood coagulating more generally, in the animals on which I have experimented, than in the human subjects who died from chloroform, is probably due to their smaller size. I was formerly of opinion that the fact of the body of a small animal cooling more quickly than the human one was the probable explanation of this, but Dr. Richardson appears to have proved that the blood is kept in a liquid state by the presence of ammonia; and ammonia, we might expect, would escape more readily from the body of a small animal than from the human body. However this may be, it is pretty certain that the blood generally remains fluid in the human body after death from chloroform, only because it usually remains fluid in every kind of sudden death. When a patient dies slowly of illness, the body cools gradually before death takes place, and ammonia keeps exhaling in the breath, if Dr. Richardson is correct, whilst the formation of this alkali must be almost suspended. In many cases, we know that coagulation of the blood commences before the respiration and circulation have ceased. The blood which flows during surgical operations coagulates as quickly and firmly when the patient is under the influence of chloroform as at other times; and, as was mentioned above, the blood which flows from animals, just after they are killed by this agent, coagulates as well as usual; it follows, therefore, that if the coagulation of the blood were prevented by the chloroform, and not by the mere fact of sudden death, it would be by the presence of this agent in the blood after death, and not by any action which it exerted during the life of the patient.
In consequence of the prevailing opinion that accidents from chloroform depended chiefly on the condition of the [248/249] patient, the main endeavours to prevent a fatal result have taken the direction of a careful selection of the persons who were to inhale this agent. It may be doubted, however, whether this line of practice has had so much effect in limiting the number of accidents, as in curtailing the benefits to be derived from the discovery of preventing pain by inhalation. In nearly all the recorded cases of accident from chloroform, it is stated that the patients had been carefully examined, and such proofs of disease as were met with after death were chiefly those which had not been detected; and, as already has been stated, were probably not greater on an average than in the cases in which no accident happened.
I have not myself declined to give chloroform in any case in which a patient required to undergo a painful operation, whatever evidence of organic disease I have met with on careful examination; and although I have memoranda of upwards of four thousand cases in which I have administered this agent, I have not, as I believe, lost a patient from its use; the only person who died whilst under its influence having, in my opinion, succumbed from other causes, as I have already explained.
Many writers have stated that accidents from chloroform might always be prevented by a close attention to the symptoms, or to some particular symptom, as the pulse or the breathing. Several authors have attached the utmost importance to feeling the pulse, and have considered this measure of itself sufficient to avert danger; whilst others have asserted that attention to the pulse is of no use at all. Mr. Bickersteth, for instance, writes as follows, in the article from which I previously quoted. "But the pulse should not be taken as any guide during the administration of chloroform. It should be wholly disregarded except under certain circumstances, when syncope is to be feared from loss of blood during the performance of a capital operation. [249/250] The pulse is only affected secondarily in consequence of the failure of the respiration."
If the person administering chloroform was always quite sure that the vapour did not constitute more than five per cent of the inspired air, it is quite true that the pulse might be wholly disregarded. I can never produce more certain and uniform results with chloroform than when I am giving it to small animals enclosed in glass jars, where of course the pulse cannot be felt. In surgical practice, however, where the amount of vapour in the inspired air is often very uncertain, watching the pulse may be of great service, irrespective of loss of blood; and although it will not always prevent accident, I am persuaded that it has saved many lives. In some of the accidents that have happened, the pulse has ceased suddenly, whilst it was being very carefully watched; but more usually it would show some signs of failure before entirely ceasing.
In giving chloroform freely to animals from a napkin or sponge, whilst the ear or the hand was applied over the heart, I have usually found that its pulsations became embarrassed and enfeebled before they ceased; and by withdrawing the chloroform when the heart's action first became affected, the life of the animal could often be saved.
The importance of attending to the respiration of the patient has been previously noticed, and it is so obvious a symptom that it can hardly be disregarded, if anyone is watching the patient; it speaks, moreover, almost to one's instincts, as well as to one's medical knowledge. It is probable that no patient has been lost by disregard of the respiration, unless it be one or two whom no one was watching, or in which the head and shoulders were covered with a towel.
It has already been shown in this work, from experiments on animals, and from the physiological effects and physical [250/251] properties of chloroform, that accidents from this agent would arise by its suddenly paralyzing the heart, if it were not sufficiently diluted with air; and a careful review of all the recorded cases of fatal accident shows that nearly every one of them has happened in this way, and not from any neglect in watching the symptoms induced, or mistaking their import.
The first rule, therefore, in giving chloroform, is to take care that the vapour is so far diluted that it cannot cause sudden death, without timely warning of the approaching danger; and the next rule is to watch the symptoms as they arise. A description of those symptoms, and what they indicate, has already been given.
I have previously stated that the most exact way of giving chloroform to a patient is to put so much of it into a bag or balloon as will make four per cent of vapour when it is filled up with the bellows; but I have not often resorted to this plan, on account of its being somewhat troublesome. I have previously described the inhaler which I employ. By arranging the bibulous paper suitably, and by ascertaining, with the inhaler in the scales, how much chloroform a given quantity of air carries off at different temperatures, I am able to produce very uniform results in the administration of chloroform. But, as I previously stated, those who do not wish to have the trouble of studying a suitable inhaler, may give chloroform on a handkerchief without danger, and with results sufficiently certain, by diluting this agent with an equal measure of spirits of wine. As the spirit (nearly all of it) remains behind, it is desirable, in a protracted operation, to change the handkerchief or sponge, now and then, for a dry one.
It is probable that artificial respiration, very promptly [251/252] applied, will restore all those patients who are capable of being restored from an overdose of chloroform. All the patients who are related to have been restored after this agent has occasioned a complete state of suspended animation, have been resuscitated by this means. It is only by artificial respiration that I have been able to recover animals from an overdose of chloroform, when I felt satisfied that they would not recover spontaneously. And under these circumstances I have not been able to restore them, even by this means, except when a tube had been introduced into the trachea, by an incision in the neck, before giving them what would have been the fatal dose.
M. Ricord succeeded in restoring two patients who were in a state of suspended animation by mouth to mouth inflation of the lungs. The first was a woman, aged twenty-six, who had been made rapidly insensible by a few inspirations of chloroform from a sponge. He had scarcely commenced the operation of removing some vegetations, when his assistant informed him that the pulse had ceased. The breathing also ceased about the same time.
In the second case, he completed the operation of circumcision, and the patient, a young man, not coming to himself, M. Ricord found that the breathing had ceased, and the pulse was becoming more and more extinct, and very soon ceased entirely, till restored by the artificial respiration.
After these cases, hopes were expressed that M. Ricord had discovered the means by which all patients might be restored from the overaction of chloroform; but these hopes have not been verified by events. In the first of the cases, the heart had probably not been so entirely paralyzed by the action of the vapour as sometimes happens, and in the second case, that organ was apparently not paralyzed by the chloroform at all. It was only after the breathing had ceased, that M. Ricord found the pulse was failing. This [252/253] was a case, therefore, in which artificial respiration might reasonably be expected to restore the patient.
The following cases of resuscitation, from the over effects of chloroform, are related by Mr. Bickersteth in the paper previously quoted. They occurred in Edinburgh:
"Case 1. A boy was cut for stone by my friend Mr. Hakes, on the 29th of March, 1849. Chloroform was administered on a piece of sponge, and the full anæsthetic effect produced, before proceeding to tie him up in the ordinary position: the inhalation was continued, without any regard to his condition, until the operation had been completed--altogether about five minutes from the time he first became insensible. It was noticed that during the operation scarce a drop of blood escaped. When it was over, the child was found, to all appearance, dead; the muscles were flaccid; the surface of the body pale; the respiration had ceased; the pulse could not be felt; the heart sounds were not audible (but the room was by no means quiet); the eyes were half open; the jaw dropped; the pupils dilated; and the corneæ without their natural brilliancy. Several means were tried to resuscitate him, but without effect. At length artificial respiration was commenced; the air escaped with a cooing sound, as if from a dead body. After continuing it for a while, the breathing commenced, at first very slowly and feebly. Soon it improved. In two hours the child had quite recovered."
"Case 2. In December 1851, a child, a few months old, was put under the influence of chloroform for the purpose of having a nævus removed from the right cheek. As soon as insensibility was produced, the operation was commenced--the handkerchief containing the chloroform remaining over the face, as some difficulty had been experienced in keeping up the anæsthetic effect. Suddenly the breathing ceased; the muscles became flaccid; the countenance pale and col-[253/254]lapsed, and the lips of a purple colour. Artificial respiration was employed, and in less than a minute the breathing returned, and the child was restored."
"Case 3. On the 6th of March, 1852, I had occasion to remove the finger of a robust, healthy-looking young man, in the Royal Infirmary. He was already under the influence of chloroform when I entered the room, and as there had been some difficulty in producing complete anæsthesia, and the last of the chloroform in the bottle was already on the handkerchief, it was thought advisable by my friend in charge of its administration to keep up the inhalation, in order to produce a coma sufficiently profound to last until the completion of the operation. It was therefore left over his face, and I commenced and removed the finger, slowly disarticulating it from the metacarpal bone. I distinctly recollect hearing the man breathing quickly and shortly; and I also remember, that when just about to look for the vessels, my attention was attracted to his condition, by not any longer hearing the respiration. The handkerchief was still on his face. I took it off, and found, to my consternation, that the breathing had ceased; the face was livid; the eyes suffused; the pupils dilated; the mouth half-open. He was to all appearance dead; still the pulse could be distinguished as a small, hardly perceptible thread, beating slowly. Immediately artificial respiration was commenced. For a minute or two, his condition did not alter in any respect--then the lividity of the countenance increased, the pulse was no longer perceptible, and the sounds of the heart could not be satisfactorily heard. During the whole of this time, artificial respiration had been diligently employed, but still the air appeared to enter the chest very imperfectly. I despaired. I felt certain that the man was dead, and that no human aid could restore him; and if it had not been that those standing near me urged me to persevere, I [254/255] believe I should then have deserted the case as hopeless. Just at this time it occurred to me to put my finger in the mouth and draw forward the tongue, in order to secure there being no impediment to the air entering the lungs. Retaining it in this position, we again began the artificial respiration, and found that then the chest was fully expanded by each inflation. After keeping it up for a minute or two, the gentleman, who had all along kept his hand on the pulse, exclaimed, to our delight, that he could again feel it--'It was just like a slight flutter that reached the upper-most of his four fingers,' all of them being placed over the course of the artery. It gradually became more distinct and firmer, and at the same time, the lividity of the face decidedly lessened. In another minute, the man made a slight inspiratory effort. I ceased directly the artificial respiration, and merely assisted the expiration by pressure upon the ribs. Another and another inspiration followed, and in a short time he breathed freely without assistance. The countenance became natural, and he appeared as if in a sound sleep. In half an hour, he spoke when roused; then he vomited, and complained of giddiness. In an hour afterwards, he had recovered sufficiently to walk home.
"Moments of intense anxiety appear much longer than they really are; but even allowing this, I am quite, sure that, at the very least, five minutes elapsed from the time when the man ceased breathing before the first inspiratory effort took place, and that for not less than one minute the pulse was imperceptible, and the heart's action almost, if not altogether, inaudible."
"Case 4. A few weeks after the occurrence just described, I was assisting Mr. Syme in removing the breast of a lady. A gentleman, my superior in the hospital, was conducting the inhalation of chloroform. Anæsthesia was complete, and the breathing good, when the operation commenced. [255/256] The chloroform was allowed to remain over the face during the whole time of its performance. Before it was over, I noticed the respiration become very quick and incomplete, and suggested, in consequence, the propriety of removing the handkerchief. My remark was neglected for eight or ten seconds, and then, just as it was taken away, the breathing ceased suddenly. The face became deadly pale; the eyes vacant; the lips livid. Instant dissolution appeared inevitable (the pulse was not felt). Artificial respiration was immediately commenced, but the air not entering the lungs freely, the tongue was pulled forwards, and retained so by the artery forceps. The chest then expanded freely with each inflation, the air escaping with a cooing sound. In rather less than a minute, the respiratory movements recommenced, but at first so slowly and imperfectly that it was necessary to assist expiration. When recovery was a little more established, the operation was completed. Before the putting in of the sutures, sensation had partially returned, and in a short time the lady had perfectly recovered."
Mr. Bickersteth very properly adds: "There can be no doubt, that in the foregoing cases, a grievous error was committed by continuing the inhalation after anæsthesia was produced, and that it was in consequence of this, the accidents, so nearly fatal, occurred."
As these accidents seem to have occurred from continuing the inhalation too long, they differ entirely from nearly all those which were actually fatal, and which, as we have seen, arose from the too great concentration of the vapour, and not from any want of care in watching the patient, so as to be able to leave off at the right moment, if it were possible. I have previously stated, that after breathing vapour of the proper strength for inhalation, animals may always be readily restored by artificial respiration after the [256/257] breathing has ceased, provided the heart is still beating. In the cases related by Mr. Bickersteth, the heart had ceased to beat before the patients were restored; but in the third case, there is distinct evidence that the heart continued to beat for four minutes after the breathing had ceased. It was, therefore, certainly not paralyzed by the direct action of the chloroform. The patient was nearly in the condition of a drowned person, where we know that there is a good prospect of recovery by artificial respiration during the first few minutes after the breathing has ceased, even if the action of the heart be imperceptible. In the other three cases, also, it is probable that the breathing ceased before the action of the heart; and, at all events, this organ was not paralyzed so thoroughly as in the cases in which artificial respiration was promptly applied without effect.
Several other cases have been related in the medical journals in which patients have been restored by artificial respiration, after animation had been suspended, more or less completely, by chloroform; but the above remarks would, I believe, be applicable to all these cases.
Where patients have recovered under the use of other measures, without artificial respiration, it is probable that animation was not completely suspended, and that the recovery was spontaneous.
M. Delarue related a case of accident from chloroform to the Academy of Medicine, on August 20th, 1850, which was apparently of this nature. After administering the vapour, and when he was about to divide some sinuses in the thigh, he found that his patient (a woman) was in a state of collapse, and the breathing and pulse, "pour ainsi dire", insensible. The face was injected, and there was a bloody froth at the mouth. The uvula was titilated, and there was immediate movement of the eyelids, which was [257/258] soon followed by copious vomiting, and the patient recovered.126
Such measures as dashing cold water on the patient, and applying ammonia to the nostrils, can hardly be expected to have any effect on a patient who is suffering from an overdose of chloroform; for they would have no effect whatever on one who has inhaled it in the usual manner, and is merely ready for a surgical operation, but in no danger. I have applied the strongest ammonia to the nostrils of animals that were narcotized by chloroform to the third or fourth degree, and it did not affect the breathing in the least. They recovered just as if nothing had been done. It is difficult to suppose a case in which the breathing should be arrested by the effects of chloroform whilst the skin remained sensible, yet it is only in such a case that the dashing of cold water on the patient could be of use. There is, however, no harm in the application of this and such like means, provided they do not usurp the time which ought to be occupied in artificial respiration; for this measure should be resorted to the moment the natural breathing has entirely ceased.
I have only seen two cases in which the patients seemed in imminent danger from the direct effects of chloroform. One of these occurred in 1853. It was the case of a child, aged six years, but small and ricketty, which had the greater part of the eyeball removed on account of melanotic disease. The usual inhaler was employed, and when the child seemed sufficiently insensible, it was withdrawn. The operation was commenced by introducing a large curved needle, armed with a thick ligature, through the globe of the eye, in order to draw it forward. As the needle was introduced, the child cried out a very little, and thinking the parents, who were in the adjoining room, would be [258/259] alarmed, I poured some undiluted chloroform hastily on a rather large sponge, and placed it over the nostrils and mouth. The sponge became pressed by the surgeon's hand closer on the nose than I intended, but it was removed after the child had taken a few inspirations. The operation was quickly concluded without any further sign of sensation than that mentioned above. At the end of the operation, the breathing was natural, but the face was pale, and the lips blue, and the limbs were also relaxed. I tried to feel the pulse at the wrist, but did not discover any. The chloroform had at this time been left off half a minute at least. The palor and blueness continued, and in a little time the breathing became slow and embarrassed, and appeared about to cease altogether, the pulse being still absent. The windows were opened, and cold water dashed freely on the face. The child made gasping inspirations now and then, but they did not follow immediately, or seem connected with each application of the water. The gasps became more frequent, till the breathing was thoroughly reestablished, when the colour returned to the lips, and the pulse was again felt at the wrist. In a minute afterwards, the child was red in the face, and crying violently from pain, which was relieved by a little more chloroform. It appeared to be a minute or a minute and a half from the time when the sponge with chloroform was removed, till the breathing became of a gasping character. There is no doubt that in this case the heart was paralyzed, or nearly so, by the chloroform, and that its action was restored by the spontaneous gasping inspirations of the child. The accident could have been prevented by having the chloroform, which was put on the sponge, diluted with spirit.
The other case occurred in the latter part of 1852. I have no notes of it, as it took place at the beginning of an illness, which prevented me from writing for some time; [259/260] but I recollect the chief particulars of it sufficiently well. The patient was a lady rather more than sixty years of age, rather tall and thin. She required to have a polypus removed from the nose. Mr. Fergusson, who was about to operate, was nearly an hour after the appointed time, and during this interval she was pacing up and down the room, apparently in a great fright. She was placed in an easy chair for the operation, and the pulse was small and feeble when she began to inhale. Nothing particular occurred during the inhalation, but just at the time when the patient was becoming insensible, the breathing ceased, and the pulse could not be felt. She appeared to have fainted, and was immediately placed on a bed which was in the room. I applied my ear to the chest, but could hear no sound whatever. Mr. Fergusson applied his mouth to that of the patient, and with a very strong expiration, inflated her lungs, so as to expand the chest very freely. I immediately heard the heart's action recommence with very rapid and feeble strokes, as I had so often heard it recommence in animals. The patient soon began to make distant gasping inspirations, and the natural breathing and pulse were soon reestablished. Mr. Fergusson made only one or two inflations of the lungs after the first one, which of itself was the means of restoring the patient. It was about twenty minutes, however, before she became conscious; and during the greater part of this time there were spasmodic twitchings of the features and limbs on one side. In about an hour, she was pretty well; and on the following day the operation was performed without chloroform.
The most ready and effectual mode of performing artificial respiration is undoubtedly the postural method, introduced by Dr. Marshall Hall a little time before his death. It consists in placing the patient on the face and making pressure on the back; removing the pressure, and turning [260/261] the patient on his side and a little beyond; then turning him back on the face and making pressure on the back again; these measures being repeated in about the time of natural respiration.
Whether the artificial breathing is successful or not must depend chiefly on the extent to which the heart has been paralyzed by the chloroform, as was previously observed. The fact of the breathing continuing after the action of the heart has ceased, in some of the fatal cases, shows that the heart may be so paralyzed as not to be readily restored by the breathing. It is probable that in all cases in which artificial respiration can restore the patient, its action would be very prompt; still it is desirable to persevere with this measure for a good while.
As already stated, there is every reason to conclude that the right cavities of the heart are distended with blood, in all cases of suspended animation by chloroform, and therefore it would be desirable to open one of the jugular veins if the artificial respiration does not immediately restore the patient. In opening animals, just after death from this agent, I have observed the contractions of the heart to return, to a certain extent, when the distension of its right cavities was diminished by the division of the vessels about the root of the neck. Opening the jugular veins has been resorted to in a few of the cases of accident from chloroform, but hitherto without success.
I have not succeeded in restoring an animal from an overdose of chloroform, by means of electricity, in any case where I felt satisfied that it would not recover spontaneously; and I have not heard of any patient being restored by its means. For keeping up respiration, mechanical means, such as the postural method, are better; as they cause air to enter the lungs without exhausting the remaining sensibility. If electricity be used, it should be directed [261/262] towards restoring the action of the heart. It is probable that the electric current would not reach the heart without the help of the acupuncture needle; but it would be justifiable to use this in a desperate case, when other measures had failed. The needles should be coated with wax, or some other non-conductor of electricity, except near the points.
In the fatal cases Nos. 40 and 48, previously related, the action of the heart partially returned during the efforts that were made for the restoration of the patient, but did not become thoroughly reestablished. It is probable that the circulation through the coronary vessels of the heart was not restored in those cases, or else the blood which must have been freed from chloroform, in its passage through the lungs, would most likely have enabled the heart to recover completely. Dr. Cockle has expressed the opinion, which is very probable, that the blood enters the coronary arteries in a retrograde manner, during the diastole of the ventricles, when the aorta and other great arteries are contracting on their contents; if so, with a very feeble circulation, the elasticity of the aorta, perhaps, cannot sufficiently act to cause a backward current; and perhaps, also, the over-narcotism of the heart is itself an obstacle to the coronary circulation, on account of the congestion of the capillaries which always attends on narcotism.
The knowledge how seldom anything effectual can be done for a person who has inhaled a dose of chloroform from which he would not spontaneously recover, ought to impress the rule very strongly on every one, to use the greatest care in its administration. [262/263]
Besides the great benefit conferred by chloroform in the prevention of pain, it probably confers still greater advantages by the extension which it gives to the practice of surgery. Many operations take place in children which could not be performed in the waking state; excisions of joints and tedious operations for the removal of necrosed bone are often performed on persons who would be altogether unable to go through them except in a state of anæsthesia; and the moving of stiff joints by force is an operation now frequently performed, although it would probably not have been thought of if narcotism by inhalation had not been discovered. The surgeon also obtains the ready assent of his patient to a number of other operations, where it would either not be obtained at all, or not at the most favourable time, if the patient had to suffer the pain of them.
The effect of chloroform cannot fail to be favourable, to a certain extent, in large operations. The patient is in a more tranquil and cheerful condition after the operation, than he would be in if he had suffered the pain of it. His pulse is usually of the natural frequency; and after an amputation, there is generally an entire absence of the starting of the stump, which was formerly so distressing. After all the minor operations in which chloroform is used, and which according to my experience comprise at least one-half of the cases, there is never a death; and the only inconvenience is a troublesome sickness of stomach in a very few instances. Moreover, when patients die after the more formidable operations, they succumb to causes which are well known, and were in operation before the practice of anæsthesia. I only know of a very few instances where there has been a reasonable doubt on the mind of the sur-[263/264]geon, whether the chloroform may not have had some share in preventing the recovery of the patient, after a severe operation. These were cases in which the sickness, which occasionally follows chloroform, continued for three or four days, indeed till the death of the patient. This is a point which it would be difficult to decide, for the latter part of the sickness might depend on the sinking state of the patient, and might have come on if chloroform had not been used. Moreover, as sickness is seldom very prolonged after chloroform in minor operations, except in persons who are not in a good state of health, it is most probable, that the patients who died after a great operation with continued sickness, would not have done well if no chloroform had been used.
Some attempts have been made to determine, by statistical inquiry, whether the result of operations has been more favourable since the introduction of anæsthesia. These attempts have been confined to the larger amputations, as they are the only operations which sufficiently resemble each other to admit of the application of statistical inquiry; and even in the case of these operations, the inquiries which had been made previously to the introduction of etherization differed widely in their results.
Dr. Simpson took great trouble, in the early part of 1848, to collect the account of the amputations of the thigh, leg, and arm, which had been performed under the influence of ether or chloroform in forty-nine of the hospitals in Great Britain; and for comparison, he collected from thirty British hospitals the results of the same amputations, for the two or three years preceding 1847. He found that the mortality in the period preceding the use of ether was 29 per cent in these amputations, and the return of patients whose limbs had been amputated under the use of ether and chloroform gave a mortality of 23 per cent; and he con-[264/265]cluded that 6 per cent of the lives of those who had undergone these amputations had been saved by the use of these agents. In his application for an account of cases, however, Dr. Simpson merely asked for the number of cases, and the number of deaths. Nothing was said as to the time when the amputations had been performed; and there is reason to believe that a number of cases still under treatment may have been included; some of which may have ended fatally after the returns were made. The cutting part of a large amputation is of very short duration. The loss of blood is not great; and patients hardly ever died during the performance of an amputation, but some time afterwards, of diseases which ether and chloroform have not been found capable of preventing. It was therefore not to be expected that these agents should save the lives of so many as 6 per cent of those who underwent the larger amputations.
In the early part of 1849, I published an account of fifty-five amputations of the thigh, leg, and arm, in which I had administered ether or chloroform, and the mortality was 27 per cent.127
Dr. James Arnott has lately been investigating this subject in a very persevering manner. During the last three or four years, all the cases of amputation performed in the London hospitals have been reported in the Medical Times and Gazette, together with their results; and Dr. James Arnott has stated that the average per centage of deaths, after the three kinds of amputation above mentioned, is 34.4 per cent. There is obviously no means of ascertaining what was the mortality after amputations in the hospitals of London before the use of ether and chloroform, but Dr. James Arnott brings forward four papers, which state the mortality for a short period, in four hospitals, a little time before the introduction of etherization. The number of [265/266] cases in these papers is 174, and the number of deaths 41. Dr. James Arnott states the per centage of deaths to be 21.9,128 although it appears to me that it would be 23.5; and it may be remarked that the four papers from which these numbers are taken might probably not have been published if the numbers they contain had not been favourable. Dr. James Arnott, in a second table, gives the number of amputations and deaths from the several hospitals in London which are named. The cases are said to have occurred "during eighteen months from June 1855 to June 1856, inclusive;" here being obviously a mistake. The number of cases is 204, and the number of deaths 61; which would give a mortality of 29.9 per cent; almost exactly the same as that which Dr. Simpson had obtained from thirty provincial hospitals before the use of ether. The numbers in Dr. Simpson's table are 618 cases, and 183 deaths, or 29.6 per cent. Dr. James Arnott does not, however, mention the per centage of deaths in his second table, but gives another table, for a different period, in which the names of the hospital are not given. The numbers he gives in this table are 430 cases and 148 deaths, giving a mortality of 34.4 per cent. Dr. James Arnott therefore concludes that chloroform causes the death of upwards of 12 per cent of those who inhale it for the purpose of undergoing amputation. It is evident that he can have had no experience of the effects of chloroform, or he would have perceived at once the error of his conclusions, for this agent is given for a much longer time than in amputations, in numerous operations of which the entire mortality is less than 12 per cent. In the removal of tumours of the female breast, for instance, more chloroform is generally administered than in an amputation, and the loss of blood is also much greater, yet the entire mortality after this operation [266/267] is considerably less than that which Dr. J. Arnott supposes that chloroform adds to the ordinary mortality after amputations.
Dr. J. Arnott stated that the pyæmia [pyemia; a form of septicemia, sometimes termed metastatic infection], of which many of the patients died after amputation, had probably been rendered more prevalent and fatal by the use of chloroform; but Mr. Thomas Holmes, in one of his able replies to the remarks of Dr. Arnott, points out that pyæmia had been prevalent also in cases of compound fracture, and others in which the patients had no chloroform. He stated that this complaint had been more prevalent in St. George's Hospital during the three years in which Dr. J. Arnott's statistics of amputations had been collected, than in the previous five years, in which chloroform had been used.129
A very valuable paper on the result of operations performed in the Newcastle Infirmary, before and since the use of ether and chloroform, was published last year by Dr. Fenwick.129a He says, respecting his tables, "in the first series are included the operations registered in the operation books of the Newcastle Infirmary from 1823 to 1843; but, as the record is imperfect, the actual period embraced is seventeen and a half years. In the second, are the operations registered since the first employment of ether and as the use of anæsthetic agents has been general in all the more important operations since that time, these figures may be used to show any disadvantages likely to arise from the employment of chloroform." Dr. Fenwick continues: "Before the use of chloroform, there were registered 225 amputations of the thigh, leg, and arm, of which 54, or 24 per cent, died. Since the use of anæsthetic agents, 149 cases of similar operations have been recorded, of which 36 died, showing also a mortality of 24 per cent. [267/268]
"Before, however, we can draw any conclusion from such facts, we must carefully exclude all those circumstances which are already known to produce an effect upon the mortality of amputations. It is, for instance, well known that amputations performed on account of accidents are, on the whole, nearly twice as fatal as those required for long standing disease. Now, if we divide the foregoing numbers into these two classes, we shall find that before the introduction of chloroform there were 144 pathological amputations, with a mortality of 19 per cent; while since its employment there have been only 61, of which 13 per cent have died; and while of 81 traumatic amputations which took place in the former period 32 per cent died, only 31 per cent perished in the latter period. The equal mortality obtained from a general average of all amputations is thus seen to have arisen from the smaller comparative number of operations performed for diseases."
After giving a table which shows the result of each kind of amputation in the two periods, he adds, "It is plain from the above table that since the employment of chloroform there has been a diminution of mortality; thus in amputations of the thigh for disease there has been 5 per cent less death, while after accidents 17 per cent have been restored to health, who formerly would have perished. In the pathological amputations of the leg there is a difference of 8 per cent in favour of chloroform; and while one out of three died after the removal of the forearm for accidents in the former series of cases, no death had occurred out of eight in the latter. The only exceptions are to be found in the traumatic amputations of the leg, and in the pathological amputations of the arm. In the former there is an excess of deaths since the introduction of chloroform amounting to 5 per cent; and in the latter, the cases, being [268/269] only two in number, do not warrant us in drawing any deduction from them."
Dr. Fenwick found that the mortality from lithotomy had been greater since the introduction of chloroform than before, but that the increase was confined to the cases occurring in adults; and he justly attributes this to the fact of the more favourable cases having been operated on by lithotrity. He says, "However paradoxical it may appear, I believe that as surgery improves the general average of mortality, both after amputations and lithotomy, will increase; in the former, from the operation being confined more and more to those suffering from accidents, and in the latter, from those with a healthy condition of the kidneys and bladder being selected for the action of the lithotrite, and the worst cases only submitting to the knife."
Dr. Fenwick gives a table showing the causes of death in the fatal cases of lithotomy before the use of chloroform and afterwards, by which it is seen that, in the latter set of cases, a larger proportion of the patients had been afflicted with organic disease, in addition to the stone. He says:--"This table shows that the relative proportion of deaths arising from the operation in healthy persons has diminished since the use of chloroform, 58 per cent having died in the former, and only 47 per cent in the latter."
Dr. Fenwick inquires into the result of a considerable number of operations in the Newcastle Infirmary, before and after the use of chloroform, in addition to those mentioned above; and gives the following summary towards the end of his paper.130 "We find that there has been a decrease in mortality since the introduction of chloroform in the following operations:-- [269/270]

Dr. Fenwick very properly remarks that other circumstances may have had an influence over the mortality of the various operations, as well as the fact of chloroform being used or not used: but his inquiry is very important, as it shows the result of operations in the same institution since the employment of ether and chloroform, and for a long period immediately preceding the use of those agents. [270/271]
General directions for the exhibition of chloroform have already been given, but it is desirable to say a few words regarding its employment in some of the individual operations of surgery.
Lithotomy. In this operation, it is advisable to have the patient placed on the operating table with his head supported by one or two pillows, and to administer the chloroform before the sound is introduced. This having been done, it is generally requisite to administer a little more vapour cautiously and gently, whilst the bandages are applied to the hands and feet, and the patient is drawn down towards the foot of the table. The bandaging should on no account be neglected in the adult patient. It would be an abuse of chloroform to carry its effects so far in every case that the slightest contraction of the muscles could not be excited by the use of the knife, merely to save the trouble of applying a bandage. In little children, the bandages are not usually employed; but in these cases, the person administering the chloroform should hold the head or shoulders of the little patient, just as the surgeon makes his first incision; for the two assistants who are holding the legs, and think they are doing a great deal of good, are really making a fulcrum to enable the child to push itself away from the surgeon, if it makes the least flinch, which it is almost sure to do, if the narcotism is not much deeper than there is any occasion for. In this operation the patient should be fully insensible when the surgeon makes his first incisions; and the chloroform must be repeated or not during the operation as occasion may require.
I have memoranda of fifty-seven cases in which I have administered chloroform in the adult, and thirty-four in [271/272] children, down to the present time, the end of March 1858. It was my expectation that I should be able to give the result of these, and all the other important operations; but I have in a few cases either not ascertained whether the patient recovered or not, or have neglected to make a note of the circumstances at the time; and although the deficiencies might perhaps be made up by private correspondence, and by searching the books of three hospitals, I regret that I have not time at present for such an undertaking.
A large proportion of the above cases of lithotomy were performed by Mr. Fergusson, either in his private practice, or in King's College Hospital, and the remaining operations were performed by a number of surgeons. On April 19th, 1855, Mr. Fergusson removed eight calculi, as large as pigeon eggs, from the bladder of a gentleman, aged sixty-nine, who had a favourable recovery.
On June 7th, in the same year, he removed fourteen calculi from the bladder of an elderly gentleman, who also recovered. In January 1857, he removed forty-two calculi from the bladder of a gentleman, aged sixty-six; twelve of them were nearly as large as ches[t]nuts, and the rest about as big as hazel-nuts. This patient died, I think, within, a fortnight. He had disease of the kidneys. A considerable number of the elderly men on whom lithotomy has been performed have had well marked symptoms of fatty degeneration of the heart; but the chloroform has acted favourably on all of them. In January 1853, Mr. Fergusson performed lithotomy in the country on a gentleman, aged sixty-four, removing a rather large calculus. The patient weighed eighteen stone; he had a pulse which was liable to intermit, some of his relations had died suddenly, and his usual medical attendant was very much alarmed about the chloroform; but its action was very satisfactory. The patient recovered his consciousness without sickness, or any [272/273] unpleasant symptom; and he had a favourable recovery. On August 11th, 1855, I administered chloroform in King's College Hospital to a man, aged seventy-five, whilst Mr. Fergusson performed lithotomy. The patient had suffered from apoplexy a year before; he was still paralyzed on one side, he had the arcus senilis well marked in both eyes, and the temporal arteries were very thick and rigid. He went through the operation well; the pulse being good all the time. He died on the fifth day, and the following appears in the Medical Times and Gazette respecting the appearances found after death. "At the autopsy, the cellular tissue of the pelvis was found infiltrated with pus. The kidneys were contracted, and occupied by many cysts; the ureters were inflamed and contained pus. The bladder was extensively sacculated, and its mucous membrane so much congested as to appear on the point of sloughing. There was no peritonitis. The heart was large and fatty, and its aortic valves diseased to a small extent. The brain was congested, and its blood-vessels extensively ossified." On December 22nd, 1855, I administered chloroform in King's College Hospital to a very fat man, aged sixty-one, with a soft weak pulse, and arcus senilis of the cornea. Mr. Fergusson performed lithotomy. He went well through the operation, and recovered promptly from the effects of the chloroform. He died on the seventh day, with purulent effusion into the left knee, and around the left shoulder. The heart was large and flabby, and the substance of the left ventricle was very friable. The right ventricle was dilated and thinned, and its walls were soft and friable, and encroached on externally by fat; at one place there seemed scarcely any muscular substance left.
I have memoranda of four cases of lithotomy in the female, in which the urethra was divided as well as dilated [273/274] to extract the stone; and I recollect two other cases of the same kind of which I have no notes.
Lithotrity. I have memoranda of 155 operations of lithotrity in which I have administered chloroform. The number of cases of stone in which these operations took place was sixty, but some of the patients had operations performed, either without chloroform, or when it was administered by some one else. The earliest cases of lithotrity in which I administered chloroform were in St. George's Hospital, and a great number of the patients to whom I have given it were the private patients of Mr. Fergusson, who is entirely satisfied of its utility in this operation. Speaking of this operation in his Practical Surgery (third ed., p. 800), he says: "I am of opinion that there is not any department of practical surgery in which anæsthesia has been of more service than in this." I have administered chloroform in a few operations of lithotrity by Sir Benjamin Brodie; but I believe that he does not approve of it in this operation, as a general rule. The following are amongst the other surgeons whom I have frequently assisted by giving chloroform in this operation: Mr. Cæsar Hawkins, Mr. Cutler, Mr. Coulson, Mr. Charles Hawkins, and Mr. Henry Lee. Mr. Fergusson, in one of his operations, extracted some portions of gutta percha bougie round which a phosphatic calculus had formed. He was not informed of the presence of the bougie in the bladder, until it was extracted. On another occasion, a patient was brought from the country soon after a bougie of this description had broken off, and he extracted with the lithotrite the piece remaining in the bladder. It was between two and three inches in length.
It is generally desirable to make the patient quite insensible during the operation of lithotrity; and the patient sometimes groans during its performance, when he is in a [274/275] condition that, so far as one can judge, he would show no sign of sensation under the use of the knife; but he, of course, has no recollection of the operation afterwards. The bladder is sometimes apt to expel the water which is injected, if the patient is not well under the influence of the chloroform; but when the vapour has been continued for a few minutes, and the narcotism is complete, the bladder will, I believe, always hold water as well as if the operation were performed in the waking state, and generally much better. There are some surgeons who occasionally raise the breech of the patient for a short time during this operation, so that the head becomes considerable lower than the body. Stout old men generally snore more loudly when in this position under the influence of chloroform; but I have not met with any ill effects, nor expected any, from the head being lowered for a short time. From ten to twenty minutes has been the most usual duration of the operations under chloroform at which I have been present.
I have administered chloroform six times in female children whilst Mr. Fergusson performed lithotrity. The patients were three in number. I think the calculus all came away after the first operation, and the second was only an examination of the bladder. I administered chloroform also, on one occasion, to a lady whilst Mr. Spencer Wells repeated the operation of lithotrity.
Section of the Urethra in the Perinæum. I have notes of 56 cases of this operation. A great proportion of them were performed by Mr. Fergusson, either in King's College Hospital, or in private practice. Amongst the other surgeons whom I have assisted in this operation were the late Messrs. Guthrie, Bransby Cooper, and Avery. In a great number of the cases, it was impossible to get a catheter into the bladder until after the incision was made in the peri-[275/276]næum, and many of the operations were very tedious; several of them lasting above an hour. It is very desirable to apply the bandages in this operation, as in that of lithotomy, especially if the assistants are not numerous.
Other Operations for Stricture, etc. I have notes of four operations in which the stricture was divided internally by a urethratome; and of two operations in which the orifice of the urethra was enlarged; and of nine plastic operations to restore deficiencies of the walls of the urethra, congenital or otherwise. I have memoranda of 66 cases in which I have administered chloroform for sounding the bladder or the introduction of a catheter. In catheterism under chloroform the patient, of course, lies on his back, which is indeed the position in which he ought to be during this operation, when chloroform is not administered.
Amputation of the Thigh. This operation is often performed for disease of the knee, when the joint is in such a state of tenderness that the least motion causes great pain. In such cases, I have administered the chloroform to the patient in bed, before his removal to the operating table, and given a little more chloroform just before the operation was commenced. In King's College Hospital, I have several times given the chloroform in the ward in such cases, before the patient was removed to the operating theatre; but in St. George's Hospital, the passages and doors being wide, the patient has been carried on his bed into the theatre, where the chloroform was administered just before his being lifted on the table. In those cases in which the tourniquet is applied, in preference to pressure with the fingers, it should be adjusted as the patient is getting under the influence of the chloroform, and tightened just before the operation begins. It is desirable to keep the patient quite insensible till the limb is removed, and the femoral artery is tied; after which a little chloroform may be given when-[276/277]ever the patient shows by a slight flinch, or contraction of his features, that sensation is returning. A few patients have recovered their consciousness during the tying of the smaller arteries, and have entered into a conversation without feeling the pain, but this condition is quite the exception. I have notes of 49 cases of amputation of the thigh in which I have administered chloroform. Some of the patients, who were almost grown up to the adult age, did not know that the limb was removed till three or four days had elapsed.
Amputation of the Leg. I have notes of 31 cases in which I have administered chloroform during this amputation. The remarks made above with regard to amputation of the thigh are applicable to this operation.
Amputation of the Arm. I have only administered chloroform five times in this operation, and only in one case during the last seven years. This case was that of a boy, aged sixteen; Mr. Hancock was the operator, and the patient recovered. I have no note of the disease for which the operation was performed, but in two or three of the remaining cases, the arm was amputated on account of malignant disease of the forearm. In one of the operations, the patient was seated in an easy chair, but in the others, the patients were lying on a sofa, or operating table, with the head and shoulders a little raised.
Amputation of the arm has apparently been much less frequently performed of late years, owing to the increasing practice of performing excision of the elbow; and it appears to me that all the great amputations are much less frequently performed now than they were a few years ago. During a little more than nine months of 1847, I administered sulphuric ether in 32 amputations of the thigh, leg, and arm; and in the last ten years and four months, I have only administered chloroform in 85 of the same operations; [277/278] in the last three years, indeed, in only 16 cases; so that the practice of amputation is still diminishing. This is due to the practice of anæsthesia, which enables the surgeon to explore and to remove diseased joints and portions of diseased bone by operations that would be too long and too painful to be endured in the waking state. This circumstance confirms the remark of Dr. Fenwick, previously quoted, that the mortality after amputations may be expected to become greater, as they will cease to be performed, except after accidents, or in very desperate cases.
Amputation of the Ankle. I have notes of 15 cases of amputation at the ankle. They were chiefly performed by Mr. Fergusson, and generally in the manner recommended by Mr. Syme, or nearly so; but latterly Mr. Fergusson and Mr. Partridge have, in three or four cases, adopted the modification of this operation introduced by Prof. Pirogoff, by which a portion of the os calcis is left.
Other Amputations. I have notes of nine cases of amputation of the forearm; four of these operations were performed in 1850, and only three since that year. I have memoranda of twelve cases in which I have given chloroform whilst Chopart's or other partial operations of the foot were performed. Also of three cases in which Mr. Fergusson performed amputation at the knee, and three cases in which he performed amputation at the wrist in King's College Hospital. I have notes also of 65 cases in which I have administered it during the amputation of one or more fingers or toes.
Operations for Necrosis. Anæsthesia is of the utmost service in these operations, which are often tedious, and would be of the most painful nature. The operations are of the most successful kind of any in surgery; they usually relieve the patient from a very painful affection, and leave no mutilation. I have administered chloroform in many [278/279] cases of necrosis in which an operation could not have been undertaken without its assistance; and in a still larger number, in which the operation could not otherwise have been satisfactorily completed. I have memoranda of 197 cases of necrosis in which I have given chloroform. In 70 of these, the tibia was the bone affected; in 15 cases, the femur; in 24 cases, the humerus; in 14 cases, the radius, or ulna, or both of these bones; in 29 cases, the bones either of the carpus or tarsus, or metacarpus or metatarsus. I have notes of six cases of necrosis of the sternum; in five of these the operation was performed by Mr. Fergusson, and in one case by Mr. Solly. Great care was required in some of the cases to avoid going through into the chest with the bone nippers. There have been nine operations for necrosis of the os calcis. In one of these, Mr. Wm. Adams lately removed, along with the necrosed bone, a small bullet which had been in the bone for six years.
The other cases of necrosis comprise the upper and lower jaw, the parietal bone, the edge of the orbit, the scapula and clavicle, the sacrum, the ileum, and the phalanges of the fingers and toes.
Excision of the Head of the Femur. I have notes of five cases of this operation. They all occurred in children from eight to thirteen years of age. Three of the operations were performed by Mr. Fergusson, one by Mr. Bowman, and one by Mr. French; I also recollect assisting Mr. Henry Smith in a similar operation in a child in 1848, at a time when I did not keep any account of the operations in which I administered chloroform. In one of Mr. Fergusson's operations, he removed some diseased portions of the acetabulum.
Excision of the Elbow. There is every reason to conclude that this excellent operation has been performed more frequently in consequence of the inhalation of narcotic vapours than it otherwise would have been. I have memoranda of [279/280] 19 cases of this operation in which I have exhibited chloroform; 18 of them were performed by Mr. Fergusson, and the remaining one was performed by Mr. Coulson, whilst Mr. Fergusson was present.
Excision of the Knee. I have notes of l7 cases in which I have given chloroform during the performance of this operation. Thirteen of the operations were performed by Mr. Fergusson, two by Mr. Bowman, one by Mr. Partridge, and one by Mr. Henry Smith. This operation had been rarely performed till within the last seven years, and there is every reason to believe that it never would have been frequently performed, if the practice of producing anæsthesia had not been introduced. I shall speak of this operation again in treating of amylene.
Excision of Wrist. There have been two cases of this operation performed by Mr. Fergusson in King's College Hospital.
The Removal of Tumours of the Upper Jaw. Mr. Syme, Mr. Lizars, and some other surgeons, expressed an opinion at one time that chloroform could not be safely used in this operation, as the blood would be liable to flow into the lungs. This is not the case, however, as the glottis retains its sensibility apparently unimpaired, if the influence of the chloroform is not too deep or long continued. It is only necessary to hold the head forward now and then, when the throat is very full of blood, in order to allow the patient the same opportunity of breathing that he would require if he were awake. A good deal of blood passes into the stomach in great operations about the mouth under the influence of chloroform; and if a few drops pass into the wind-pipe, they are coughed up again, as they would be in the waking state; there is, however, less appearance of suffocation in operations where the blood flows back into the throat, when the patient is insensible, than when he is [280/281] awake. The glottis appears to retain some sensibility as long as a creature is capable of breathing, for I have placed the head of more than one cat under water after making them thoroughly insensible with chloroform, and the action of the respiratory muscles lasted more than two minutes, but no water entered the lungs.
I have always made the patient insensible in the usual way, with the inhaler, before the operation of removing tumours of the jaw, and have kept up the insensibility during the operation by means of a mixture of chloroform and spirit on a hollow sponge; or in cases in which I have not been provided with this mixture, I have put not more than fifteen or twenty minims of chloroform on the sponge at one time. Owing to the hands of the surgeon and his assistants being very much in the way, I have not always been able to keep the patient quite insensible throughout the operation. He has sometimes struggled or cried out, but there has been hardly any case in which the patient afterwards remembered any considerable part of the operation.
I have notes of twelve cases of removal of the upper jaw in which I have administered chloroform, in addition to four cases to which I alluded in the Medical Gazette, in the early part of 1849. In some of the cases, the malar bone was removed, as well as the superior maxillary. Eleven of these operations were performed by Mr. Fergusson, and the others were performed by Mr. Partridge, Mr. Henry Charles Johnson, Mr. Hewett, Mr. Henry Smith, and Mr. Haynes Walton.
Mr. Fergusson introduced a great improvement in this operation about seven years ago; instead of the incisions through the cheek or lip, or both of these parts, he merely slits open the lip exactly in the mesial line, as far as the columna of the nose, and then carries the knife along one [281/282] side of the base of the columna into the nostril, next the tumour. He says: "By opening the nostril in this way as much relaxation was gained as if the knife had been carried from the root of the ala an inch up the side of the nose, and as much facility was given for the future steps of the operation, as if an incision three inches in length had been made through the lip and side of the nose, while a grand object was gained in leaving the slightest possible conspicuous appearance afterwards."131 This plan has the further great advantage of avoiding the very copious hæmorrhage which arises from a deep incision in the side of the face.
In one of the operations which was performed before this improvement was introduced, the patient died of hæmorrhage. The case is related by Mr. Prescott Hewett in the Medico-Chirurgical Transactions for 1851. This operation was performed in St. George's Hospital, in May 1848, with the consent of the surgical staff of the hospital. The patient was a man, aged twenty-five; the tumour was of nearly six years duration. For some time previous to the operation, he had suffered occasionally from hæmorrhage from the affected nostril, to an extent which had reduced him considerably. The vapour was given to him rather slowly, with the apparatus I commonly employ, and he became gradually insensible, without previous excitement or struggling. In about three minutes, the inhalation was discontinued, the narcotism having reached the third degree. The patient was passive, but the muscles were not relaxed. The breathing was not stertorous. Some teeth were now extracted without causing any sign of pain. A little more chloroform was then given to him, and when the inhalation was discontinued a second time, he was in the same state as before the teeth were drawn. The operation was immediately commenced. The superior maxillary and malar [282/283] bones of the left side were removed. During the first part of the operation, whilst the flaps were made, the patient was perfectly quiet and silent; but afterwards he began to groan and move his limbs, and he was not again rendered altogether insensible; for although a few minims of chloroform were from time to time sprinkled over a sponge, which was, now and then, held near his face, yet, owing to the hands of the operator and his assistants being in the way, and the cavity of the mouth and nostril being laid widely open, he got very little of the vapour, and the only effect of it was partially to quiet him on one or two occasions. After the first two or three minutes of the operation, the effect of the chloroform never exceeded the second degree. The patient executed voluntary movements of his arms and legs; sometimes it was necessary to hold his hands, and at one time he appeared conscious, for he folded his arms as if making an effort not to raise his hands to the seat of pain. He coughed now and then, and seemed somewhat embarrassed with the blood in his throat. He was seated in a chair, but as there was no window in the operating theatre except the skylight, his head was obliged to be inclined rather backwards. He was leaned forwards once or twice, to allow him to get rid of the blood, and it appeared that he vomited some on one of these occasions. Towards the conclusion of the operation, and at a time when he was very little under the influence of chloroform, he fainted. He was laid down, and brandy was given to him. No more chloroform was administered after this time. He partially rallied from the syncope, but again became faint. The actual cautery was applied, but oozing of blood continued until the moment of death,--about half an hour after his removal into another room. During this interval, he was much exhausted; his pulse was small, and difficult to feel. He was tossing himself about in a restless manner, but there was no [283/284] difficulty of breathing. He seemed quite conscious, doing as he was told, but, of course, could not speak, from the nature of the operation. I left a few minutes before the patient's death. When he ceased to breathe, laryngotomy was performed, and artificial respiration exercised by the opening, with no beneficial result. In my opinion, this measure was not indicated, but of course it could do no harm.
One of the surgeons who was present when the patient died informed me that blood entered his windpipe from the wound, when he became moribund.
It was found during the operation that the tumour did not involve the superior maxillary or malar bones, but was situated behind them. In his address to the class immediately after the operation, Mr. Hewett estimated the loss of blood at sixteen ounces. It appeared to me to be much greater; besides that a great deal of blood would certainly be swallowed.
After death, portions of the tumour were found still remaining attached to the posterior and upper part of the cavity, and projecting into the foramen lacerum of the orbit and right nostril, as well as in other directions. The trachea and bronchi contained some frothy blood. Numerous small dark spots of congestion were met with in the lung, resulting from some of the small bronchi being filled with blood.
The late Mr. Liston lost a patient from hæmorrhage during the removal of a tumour of the upper jaw, before the prevention of pain by inhalation was discovered; and it is evident that the chloroform did not contribute either directly or indirectly to the death of Mr. Hewett's patient. His symptoms were simply those of exhaustion from loss of blood; he recovered from the effects of the chloroform some time before he died; and the small quantity of blood [284/285] which spotted the lungs, and was observed to enter as he was dying, would not have led to any immediate urgent symptoms if it had entered during the operation.
Tumours of the Lower Jaw. I have notes of twelve cases in which I have given chloroform during this operation. Eight of the operations were performed by Mr. Fergusson, and the others by Mr. Stanley, Mr. Tatum, Mr. Hancock, and Dr. Pettigrew. In some of the cases the jaw was divided on each side above its angles, and in most of the others it was disarticulated on one side, and divided near the symphysis. Three of the patients died within three days, from the hæmorrhage which occurred at the time of the operation, but the others all recovered.
The remarks which were made respecting the application of chloroform in the removal of tumours of the upper jaw are applicable here. After the operation has been commenced, one should endeavour to keep up the insensibility by means of a mixture of chloroform and spirit on a hollow sponge. In tumours, both of the upper and lower jaw, the operating table is preferable to an easy chair for the patient under chloroform. The head and shoulders must be raised by the moveable flap of the table, or by some other contrivance if the operation be performed in a private house. I have, however, seen the operation performed on a sofa, and with the patient in bed. The blood does not flow into the throat so much in the removal of tumours of the lower jaw, as in those of the upper one.
Tumours of the Female Breast. I have memoranda of 222 cases in which I have given chloroform during the removal of tumours of the breast, or tumours which returned after the breast had been removed. I do not include with these a considerable number of small tumours, situated upon, and near the gland, but not involving it. By far the greater number of the tumours of the breast were [285/286] looked upon as malignant, but I am not able to state the numbers which were believed to be malignant, and which were thought not to be so. I may state that there is no surgeon whom I am in the habit of assisting who does not occasionally remove malignant, as well as non-malignant, tumours of the breast. By far the greatest proportion of the above mentioned operations on tumours of the breast were performed in private practice. In a number of cases diseased glands were removed from the axilla, in addition to the mammary gland. It is desirable in the removal of large tumours of the breast that the surgeon should be well seconded, by assistants who are in the constant habit of assisting him, in order that the bleeding may be restrained and arrested as quickly as possible. I have not seen any case in which the patient did not go through the operation, and live, as far as I can remember, for two or three days. But a few of the patients have been very faint from bleeding during the operation, and faintness from hæmorrhage seldom takes place during the influence of chloroform unless the loss of blood is very great. The greater portion of the patients who have been faint during the operation have done well afterwards, but a few of them have not. In cases where there is a great loss of blood, and a very large wound remains, the patients are apt to sink and die in from three to five days. Most patients may recover from a considerable hæmorrhage, and most patients may be able to bear up during the healing of a large wound, but the combination of a great hæmorrhage and a great wound is apt to be fatal; especially to patients who are already reduced by illness. The largest tumour of the breast I have seen removed, was one on which Mr. Fergusson operated, in King's College Hospital, on Feb. 26th, 1853; it weighed eighteen pounds and a half. On the 4th of June, following, the same patient had a small tumour removed from the [286/287] same situation. It probably resulted from a portion of the large one which had been left behind.
There area few surgeons who prefer to have the patient seated in an easy chair whilst removing a tumour of the breast but it is more convenient, under the influence of chloroform, that the patient should lie on a table, or sofa, or in bed. I usually keep the patient unconscious till the wound is stitched up, and the plaster and bandage applied.
I have administered chloroform in four cases of tumour of the male breast. These tumours were all of them malignant, I believe.
Other Tumours. I have had to administer chloroform during the removal of several large and deep-seated tumours of the face, situated just in front of the ear, over the parotid gland, with which some of them were thought to be connected. These operations were generally extremely difficult and tedious, owing to the necessity of avoiding the division of the branches of the facial nerve which passed over the tumour. When the branches of the facial nerve are touched with the forceps, or back of the scalpel, during these operations, the muscles of the face to which the branches are distributed contract very freely, at a time when the patient is perfectly insensible. Mr. Stanley, Mr. Fergusson, and Mr. Tatum, are amongst the surgeons whom I have assisted in the removal of tumours of this kind.
I have memoranda of 41 tumours situated behind the angle of the jaw, in the removal of which I have exhibited chloroform. These tumours, which mostly consisted of diseased lymphatic glands, were often very deep-seated, passing near to the carotid artery, and it was necessary on that account to keep the patient quite insensible, to prevent his flinching during the operation. The greater number of these tumours were removed by Mr. Fergusson.
Seventy-one of the tumours of the removal of which I [287/288] have notes, are stated to have been of the encysted kind. Sixteen of them were situated on the eyelids, sixteen on the scalp, three or four in the orbit, several in front, or at the side of the neck, and the rest in different parts of the body.
I have memoranda of 66 fatty tumours which were removed from different parts of the body. Some of them were of great size; one weighed fifteen pounds. One which Mr. Fergusson removed in 1855 from the arm of a lady, the patient of Messrs. Maurice and Harris of Reading, was situated beneath the biceps muscle, and weighed two pounds six ounces and a half. The diagnosis of it was very difficult. The fatty tumours were easily removed, except in a few instances, in which the fat was infiltrated in the surrounding tissues.
I have notes of the removal of 87 other tumours of various kinds, as fibrous, scirrhous, epithelial, melanotic, fungoid, etc.
On February 11th, 1854, Mr. Fergusson removed a large fibrous tumour, situated over the right scapula of a stout gentleman about forty. It weighed about three pounds. The tumour was very adherent to all the surrounding tissues, and the removal of it occupied five or ten minutes, and was attended with considerable hæmorrhage. At the time when the tumour was completely detached, the patient became pale, and the pulse could no longer be felt in either wrist or in the temporal arteries. He did not faint, however, for the breathing continued to be well and regularly performed. He partially recovered his feeling once or twice, whilst the vessels were being tied, and more chloroform was given to him. At the end of the operation he was quite conscious, and did not complain of being faint, although no pulse could be felt. The pulse had not returned when I left him half an hour after the operation, and I was informed that it did not return for about three [288/289] hours. Four hours after the operation, when I called to see him, he had a frequent and very distinct pulse. He had some hot brandy and water just after the operation, and about ten minutes afterwards he insisted on going to the water-closet in the next room, and could not be persuaded to lie still. The moment he was raised on his feet, however, he fainted, but was immediately laid down again, when he as quickly recovered his consciousness, and was content to lie still. This was the only faintness he had. It is my opinion that the effect of the chloroform kept up the breathing and prevented syncope, whilst the smaller arteries of the exterior of the body contracted so as to confine the remaining blood very much to the vital organs. The patient seemed in some danger for two or three days, but was walking out quite well in less than a fortnight.
In April 1856, Mr. Paget removed a fibro-cellular tumour, weighing probably ten or twelve pounds, from a lady a few weeks out of her confinement. The tumour was situated over the sacrum and nates. Sir Benjamin Brodie was present at the operation. The patient recovered favourably.
Nævi. I have memoranda of 116 operations on vascular tumours, the greater part of them in infants. The operations have generally been performed by subcutaneous ligature, and have been extremely successful. The greater number of them have been performed by Mr. Fergusson and Mr. Bowman, in private practice and in King's College Hospital. Some of the nævi on the faces of infants, which were operated on by Mr. Fergusson, were very large, and required a succession of operations.
Ligature of Arteries. I have administered chloroform in three cases of ligature of the carotid artery, by Mr. Bowman, Mr. Lane, and Mr. Haynes Walton. Mr. Walton's patient was an infant six months old. The right common carotid artery was tied, on account of a tumour which [289/290] pushed forward the eye to a great extent. On the child being brought under the influence of chloroform, the prominence of the eye diminished very much, as I was informed that it had done when chloroform was given for some reason on a previous occasion. On the ligature being placed under the artery, the chloroform was discontinued, and its effects allowed to subside before the ligature was tied. As the effects of the chloroform went off, the eye became as prominent as before; and the tightening of the ligature had no effect on this prominence whilst I remained, although it instantly stopped the pulsation of the temporal artery. I was informed that this child was cured by the operation.
I have also administered chloroform in three cases of ligature of the external iliac artery, for aneurism of the femoral. Two of the operations were performed by Mr. Fergusson, and the other by Mr. Henry Smith. One of Mr. Fergusson's patients was a very stout gentleman; the external iliac artery was diseased at the usual situation of the ligature, and it had to be tied near to the common iliac. This patient died. Mr. Henry Smith's patient recovered, as I believe did the other of Mr. Fergusson's. It is necessary that the patient should be kept very insensible during the operation of tying the carotid or external iliac artery, to prevent the possibility of his flinching.
I have exhibited chloroform six times for the ligature of the superficial femoral artery, on account of aneurism in the popliteal space. Two of these operations were performed by Mr. Bowman on the same man with an interval of three weeks. He had an aneurism in the popliteal space of both limbs. There was a case of false aneurism of the radial artery, on which Mr. Fergusson operated by tying the artery above and below, and turning out the clot; and also a case in which Mr. Hancock tied the vessels for a [290/291] false aneurism, situated between the metacarpal bones of the thumb and forefinger. There were two cases also in which the radial artery was tied for a recent wound; one by Mr. Henry Charles Johnson, the other by Mr. Henry Lee.
Tumours of Bone. I have administered chloroform in a number of cases of the removal of enchondroma, and other tumours of bone. In June 1849 I assisted the late Mr. Aston Key whilst he removed a bony tumour from a youth about sixteen, situated at the inner and anterior part of the femur, just above the knee; and I have seen two or three other tumours of the same kind, exactly in the same situation. I have no notes of the other cases; but one was a patient of Mr. Quain, and another, I think, of Mr. Fergusson. After an incision is made, the tumour can be clipped clean off at once with a pair of strong, curved bone nippers. Unless the bone nippers are curved, the operation is troublesome and difficult.
Hare-Lip. I have notes of 147 operations for hare-lip, for which I have given chloroform. A few of these operations were performed by Mr. Arnott, Mr. Cæsar Hawkins, Mr. Bowman, Mr. Henry Charles Johnson, and others, but nearly nine-tenths of the whole number were performed by Mr. Fergusson, either in his private practice or in King's College Hospital. A great number of Mr. Fergusson's operations were in children from three to six weeks old; and some were younger than this, one being only eight days. There used to be an objection against operating for hare-lip on very young infants, as it was said that they often died of convulsions, which I believe to be true. The convulsions were supposed to be caused by the shock of the operation on the nervous system, which I believe to be entirely untrue. I believe they were caused by hæmorrhage; and I would not recommend the surgeon to perform [291/292] his first operations for hare-lip on very young and feeble infants. The great success of this operation of late years, in the first weeks of life, depends on the dexterity of the surgeon who performs the operation so quickly that scarcely any blood is lost. When Mr. Fergusson performs this operation, the infant is held by a nurse, who is seated opposite to him, whilst its head is placed in his own lap between his thighs. An assistant compresses the labial artery on the right side, by grasping the lip between his finger and thumb, just at the angle of the mouth; a sharp-pointed scalpel is pushed through the lip on the right side, just below the nose, and carried downwards so as to cut away the edge of the fissure; then the same performance is done on the left side of the fissure, while Mr. Fergusson compresses the labial artery on that side with the finger and thumb of his left hand. In about twenty seconds from the beginning of the operation, the hare-lip pins are introduced, and the cut edges of the lip being pressed together, the bleeding is at once entirely stopped. I have no doubt that many lives are saved by early operation, especially amongst the poor, as a child with a bad hare-lip cannot take the breast till it is operated on, and there is a very great mortality amongst infants brought up by hand.
The blood which escapes when the infant is laid on its back flows back into the throat, and it usually passes on each side of the epiglottis, and runs into the stomach without any act of deglutition. In a few cases of strong children, in whom the bleeding is rather free, the breathing gets embarrassed, and Mr. Fergusson turns the face of the child downwards for a moment to let the blood run out of its mouth. When the quantity of blood flowing into the throat is greater than can run down into the stomach, in the way I have mentioned above, the glottis closes and the breathing stops, which gives the indication for turning the [292/293] face downwards. I have seen a few operations in the hospital for hare-lip, without chloroform, whilst the children were on their backs. In these cases they cried violently from the pain, set the blood in the mouth into violent commotion, and then drawing a deep inspiration, drew a little of the blood into the larynx, which caused a violent cough; so that there was usually much more appearance of choking than in the cases where chloroform was given. Moreover, in these latter cases, it is usually towards the end of the operation that the children sometimes become embarrassed with the blood; not because the quantity of blood is greater, but because the sensibility is returning. I have seen one case which shows that the effects of chloroform, when deep or long-continued, will diminish the sensibility of the glottis. After an infant was made insensible some years ago for an operation for hare-lip, it was found that an instrument for dividing the projecting intermaxillary bone was wanting, and I kept the child insensible for several minutes, by administering chloroform occasionally, until the instrument was found; the bleeding was rather free, and some of it entered the windpipe and caused a tracheal râle. The child coughed it up on awaking, and no ill consequences followed; but the occurrence confirms the opinion previously expressed, that the insensibility should not be both deep and long-continued at a time when copious hæmorrhage is flowing into the throat. The effects of chloroform pass off very quickly in infants, and it is not often that they last till the operation of hare-lip is finished, short as that operation is. In private practice, indeed, when the parents of the infant are close by, I usually have an opportunity to apply a little chloroform, mixed with spirit, on a sponge, in the course of the operation, when it is required to prevent crying; but in the hospital, the children sometimes cry a little before the operation is concluded. [293/294]
Cancer of the Lip. I have memoranda of nineteen cases of cancer of the lower lip, and three or four of the upper lip, in which I have administered chloroform. As there is never an easy chair in the operating theatre of an hospital, and it is difficult to keep the patient in a common chair when he is under the influence of chloroform, it is better to place the hospital patient on the operating table, with his head and shoulders raised during this operation; but in private practice the patient may either be placed on a sofa, or in a large easy chair with a high back. The effect of the chloroform often lasts to the end of the operation, if it be completed within two or three minutes; but I always go provided with a hollow sponge, and a mixture of chloroform and spirit to apply during the operation, if required.
Division of the Sensory Nerves of the Face. I have notes of nineteen cases in which I have administered chloroform during this operation. They were chiefly performed by Mr. Fergusson, but a few of them by Mr. Bowman. The operation is of so painful a nature, that I believe it was seldom performed before the practice of inhaling narcotic vapours was introduced. It is done subcutaneously, by means of a small sharp-pointed bistoury, by which the affected nerves are chopped up by twenty or thirty incisions, at and near the points where they issue from their respective foramina. In operating on the mental branch of the fifth nerve, the bistoury is sometimes introduced from the face, and sometimes from the interior of the mouth. The pain continues for two or three days, till the inflammation caused by the operation subsides, when there is usually a complete absence of pain for three or six months, at the end of which time the operation has often to be repeated. I am not aware whether the relief has been permanent in any case, but it has often been very complete for a time. One patient, on whom Mr. Fergusson operated in King's College Hospital, looked like [294/295] an old man at the time of the operation, but this was the effect of his severe suffering; for a week or two afterwards he looked his real age, which I think was less than forty. This operation is not performed for the milder cases of neuralgia, or for cases that can be cured by quinine or iron; but only for the more terrible forms of the complaint, which fortunately are somewhat rare. Rare as they are, however, they occur sometimes in near relatives.
Division of other Nerves of Sensation. I have notes of nine cases in which nerves in other parts of the body were divided, and a portion cut out, for neuralgia. On four occasions the nerve was situated in a stump following amputation; and on two occasions a tumour of the nerve was removed. The operations were performed by Mr. Fergusson, Mr. Solly, and Mr. Paget.
Operations on the Eye. The operations for cataract are frequently performed without chloroform, when the patient has sufficient resolution to keep his eye steady. I have, however, administered chloroform fifty-three times during the extraction of cataract; thirty of the cases occurred in the private practice of Mr. Bowman. On November 25th, 1851, I administered chloroform whilst Mr. White Cooper extracted a piece of flint from the interior of the eye; and on February 7th, 1852, whilst Mr. Bowman extracted the capsule of the lens. On February 17th of the same year, I assisted Mr. White Cooper with chloroform whilst he extracted a cataract from the eye of an elderly lady; and I assisted him in eleven other cases during that and the following year. I assisted Mr. George Pollock in two operations of the extraction of cataract in June 1852; and Mr. Lawrence in three operations in 1853. Eighteen of Mr. Bowman's operations were performed in the summer and autumn of 1854, and were of the usual kind; but in six out of the twelve cases in which I have since assisted him, [295/296] the cataract was first drilled and then removed, in a softened state, through a small opening in the cornea, by means of a small scoop. I have assisted Mr. Alexander in two cases, and Mr. Critchett also in two. Several of the patients were over eighty years of age.
The operation for the extraction of cataract is said not to be a painful one, but the patient requires to be as insensible during its performance as if he were about to undergo lithotomy, or a great amputation; without this, the eye and eyelids will not be steady. The insensibility must be kept up completely until the cataract is extracted.
It is necessary that the stomach should be empty when the patient inhales chloroform for this operation, in order that vomiting may, if possible, be avoided. There was a little vomiting in a very few of the cases in which I administered chloroform, but it was not attended with straining, and I believe it did no harm in any case. Mr. Bowman informed me of a case of his in which chloroform was administered in the Ophthalmic Hospital for the extraction of cataract, and the woman vomited violently afterwards, and the eye was destroyed. She, however, was a person of bad constitution, and the vomiting might have occurred without the chloroform. The patients were lying on a sofa in all the operations, except, I think, one by Mr. Alexander.
I have notes of nine cases of the drilling of cataract in which I have administered chloroform, and there were some other cases in 1848, of which I have no memoranda. Some of the early operations were performed by Mr. George Pollock, and the more recent ones by Mr. Bowman. Many of the patients were infants or children. There have been two cases of the removal of coagulated lymph from the interior of the eye, by Mr. Bowman and Mr. White Cooper; and six cases of the formation of artificial pupil, by the same surgeons, and Mr. Dixon; and in two cases lately, Mr. Bowman has removed a portion of the iris. [296/297]
I have given chloroform in 25 cases of excision of the eyeball; 20 of the operations have occurred within the last two years, in addition to some in which I administered amylene. The whole of the operations were performed by Mr. Bowman, except one by Mr. Fergusson, and one by Mr. Hancock. The operation is of late years a much less formidable one than formerly, owing to the plan of commencing to dissect off the conjunctiva just around the cornea. After the eyeball is removed, the edges of the conjunctiva are drawn together by a fine suture, so that scarcely any wound is left, and the patient can generally begin to wear an artificial eye in four or five days. In cases of malignant disease extending beyond the globe, of course, the more formidable and extensive operation would still require to be performed.
I have administered chloroform for the removal of sparks of iron and other foreign bodies from the cornea, chiefly in cases in which the surgeon had previously tried without success. Under the influence of chloroform, the foreign matters were always removed very readily. There have also been operations for the removal of growths from the eye and granular growths from the conjunctiva, and also, for staphyloma and pterygion.
I have memoranda of 54 operations for strabismus in which I have administered chloroform. The greater number of them were performed by Mr. Bowman, but several by Mr. Fergusson, and a few by other surgeons. One operation was performed by the late Mr. Dalrymple. Mr. Bowman generally operates on both eyes at the same time. A great number of the patients who have taken chloroform for this operation were children. They have nearly all been lying down during the operation.
There have been nine operations for ectropion and entropion, chiefly by Mr. Bowman. I have administered chloro-[297/298]form on four occasions whilst Mr. Bowman has performed a plastic operation for the formation of a new eyelid. On three occasions, the eyelid had been destroyed by a burn, and the material for the new one was taken from the integuments of the forehead. The operations were necessarily tedious.
Removal of Foreign Bodies and Polypi from the Ear. In May 1849, Mr. Henry Charles Johnson extracted a pea from the ear of a child, six years of age. The pea had been a month in the ear, and Mr. Johnson had endeavoured to examine the ear without chloroform, but could not do so. In May 1857, I administered chloroform to a child aged three years, a patient of Mr. Tuach, whilst Mr. Hewett extracted a glass bead with sharp edges from the ear. He got it out with a director. I have notes of four cases in which a polypus was removed from the ear by Mr. Partridge, Mr. Fergusson, Mr. Henry Lee, and Mr. Henry Smith; and I recollect giving chloroform more than once at Mr. Toynbee's whilst he performed a similar operation, although I have no memoranda of the circumstances.
The Removal of Polypi and Foreign Bodies from the Nose. I have memoranda of fourteen cases in which I have administered chloroform for the removal of polypi from the nose. The operations were nearly all performed by Mr. Fergusson. The patient was nearly always seated in an easy chair, and the chloroform, in several cases, was repeated to keep up the insensibility till the operation should be completed. In one of the cases, the polypus caused a protrusion of the nasal bones; the nostril was slit up, and there was very great hæmorrhage as the polypus was brought away. The pulse became small for a time, but there was no syncope. The patient did well. In June 1852, I gave chloroform to a girl, five years old, and Mr. Fergusson scooped out some polypus growth from the right nostril, and also an oval [298/299] softened body, rather bigger than a horse-bean, which was a young orange that the child had pushed up her nose in India. The case had given rise to a good deal of difference of opinion amongst medical men in India and Malta, who generally discredited the child's account of the orange. In August 1856, Mr. Stanley removed a bean from the nose of a child.
Certain Operations in the Mouth. I have notes of six operations for cancer of the tongue, performed by the late Mr. Keate, Mr. Quain, Mr. Hancock, and Mr. Paget. Mr. Paget's was a case of epithelial cancer, in a lady, about twenty-five. The operation was one of excision of the tumour, and I lately heard that the patient remained free from the complaint. The other operations were by ligature. Mr. Quain's was a hospital patient, and I do not know the ultimate result of the case. The other patients had a return of the disease, and died after great suffering.
I have notes of ten operations for epulis, chiefly by Mr. Fergusson. The patient was generally on a sofa or the operating table, with the head and shoulders raised. As the operations were soon completed, the chloroform seldom required to be repeated. There have been some cases of cancerous disease of the gums and alveolar process in which I have administered chloroform. One of these was a patient of Mr. Bell, the dentist, on whom Mr. Hilton operated. I assisted the late Mr. Avery by giving chloroform in two operations for cleft palate. A large cork with a string to it132 was kept between the molar teeth on one side during the operation; and the inhalation was repeated from time to time. The surgeon, however, much prefers to have the patient awake during this operation, when he can get his assent. [299/300]
I have administered chloroform four times for the removal of the tonsils. Three times in children, and once in the adult. In the case of a child on which Mr. Curling lately operated, he removed one of the enlarged tonsils very easily and very well, but just as he was beginning to remove the other, the child began to vomit its breakfast, and the throat was afterwards so filled with mucus and blood, that we thought it better to defer the remainder of the operation till another day.
Plastic Operations. I have memoranda of 50 plastic operations in which I have administered chloroform, in addition to those on the eyelids, previously mentioned. Eight of the operations were for the formation of a new nose. Five of them were by Mr. Fergusson, two by Mr. Critchett when Mr. Fergusson was present, and one by Mr. Samuel A. Lane. I made the patients insensible with the inhaler before the operation was commenced, and afterwards kept up the insensibility by means of chloroform, diluted with spirit, on a hollow sponge. No fewer than 24 of the plastic operations were for the remedy or mitigation of deformity caused by burns. In fourteen of these cases, the operation was performed on the neck, but often extended to the breast and lower part of the face. The other ten operations were for burns on the face and arms and other parts of the body. Nearly all these operations were performed by Mr. Fergusson. One of his patients was a gentleman from New York, who had a most severe burn in the face when a child. The operations, without the action of a narcotic, would be of the most painful nature; and the greater number of those at which I have been present would not have been performed, except for the discovery of narcotism by inhalation. The remaining eighteen plastic operations were for a variety of purposes, such as replacing the loss of a lip, the closing of artificial anus, and of openings in the cheek, and a variety of other defects, either congenital, or [300/301] arising from injury or disease. They were nearly all performed by Mr. Fergusson.
Raising depressed Portions of Skull. In Dec. 1848, I administered chloroform to a gentleman in Norfolk, aged sixty-two, on whom the late Mr. Aston Key operated. The patient had been thrown from his horse four years previously, and probably kicked whilst on the ground. He believed that he did not lose his consciousness. There was a considerable depression of a portion of the right parietal bone, near its upper and posterior angle; but there were no symptoms of cerebral pressure or irritation for two years after the accident; but at that time he fell from his seat in some kind of fit, after which he had partial paralysis of the left arm, impaired vision, and a melancholy or apathetic state of mind. He was also subject to attacks of real or apparent suspension of breathing, and to occasional attacks of vomiting.
His ordinary medical attendant, Dr. Bell of Aylsham, objected to the chloroform, on account of feeble and irregular action of the heart, in addition to the above symptoms. The patient, however, became gradually insensible, without any unfavourable symptoms. After making incisions in the scalp, Mr. Key sawed out a good sized piece of the parietal bone with Hey's saw. The insensibility was kept up gently during the operation, which lasted above half an hour. There was pus under the bone, and the dura mater was diseased, and gave way during the operation. Mr. Key immediately expressed a bad opinion of the case. The patient recovered his consciousness in about a quarter of an hour, and in a little time was in the perfect enjoyment of all his faculties, being very cheerful, and in a totally different state from the one of apathy and almost unconsciousness, in which he appeared when we first saw him. He was attacked with inflammation of the brain on the third day, and died on the fifth. [301/302]
In May 1855, I administered chloroform in St. George's Hospital to a young man who had been kicked by a horse. The frontal bone above the right eye was driven in to a good depth, and a little of the brain had escaped. Mr. Cæsar Hawkins cut a piece from the frontal bone, just above the depressed portion, with the bone forceps, to enable him to introduce the elevator. The depressed portion being quite loose, was removed, together with the roof of the orbit. The youth was partially comatose before chloroform was given, but made a resistance to the operation. A week after the operation, when I saw him, he was conscious, but feverish, and he died a week or two later.
Mr. Bowman, on one occasion, made an incision over the frontal sinus in a gentleman; and made an aperture in the outer table of the frontal bone, which gave exit to a quantity of pus which had been formed in the sinus.
In the summer of 1847 the late Mr. Liston performed a similar operation on a lady, the patient of Dr. Locock, who was present. I exhibited sulphuric ether on that occasion.
Operations for ununited Fracture. I have notes of seven operations by Mr. Fergusson and Mr. Bowman, for ununited fracture of the femur, humerus, radius, and ulna. The usual course has been to scrape and puncture the ends of the bones by subcutaneous incision, and where this has not succeeded, to cut down on the bones and saw off the ends; or to bore holes near the ends, and introduce ivory pegs.
The Reduction of Dislocations. I have notes of twenty-seven cases in which I have administered chloroform during the reduction, or attempted reduction, of dislocations. Only three of these were recent dislocations. One had existed a few days; and the other twenty-three for some weeks or months. Twelve of the operations were performed by Mr. Fergusson, and the others by Mr. Cæsar Hawkins, Mr. Cutler, Mr. Bransby Cooper, Mr. Partridge, Mr. Tatum, Mr. [302/303] H. C. Johnson, Mr. Charles Hawkins, Mr. Hewett, Mr. Hoary Lee, and Mr. Price. Most of the dislocations at the shoulder were quite successfully reduced; one of them by the late Mr. Bransby Cooper, as long as ten weeks after the accident. Dislocations of the hip were successfully reduced in three weeks and five weeks after the accident. At longer periods, dislocations of the femur were often benefited by the operation, but not completely reduced. The dislocations at the elbow were not successfully reduced except when recent, although the position and motion of the forearm were improved in several cases by the operation. Pulleys were applied, often for a length of time, in the old dislocations; and many even of the successful operations could not have been performed except the patient had been in a state of anæsthesia. A full dose of chloroform is required in the attempts to reduce old standing dislocations, in order to suspend, as nearly as may be, the resistance of the muscles.
Forcible Movement of Staff Joints. I have given chloroform in twenty-two operations of this kind, within the last three years, for the restoration of motion in the knee, elbow, and hip, after the joints had become fixed in one position, generally by adhesions resulting from disease. The first operation of the kind in which I assisted was one performed by Mr. Brodhurst, whom I have since assisted more frequently in these kind of operations than any other surgeon; but other operations have been performed by Mr. Fergusson, Mr. Cæsar Hawkins, Mr. Partridge, Mr. Bowman, Mr. Hewett, and Mr. Edwin Canton. These operations would evidently not have been performed except for the discovery of producing a state of anæsthesia by inhalation.
Tenotomy. I have memoranda of 78 cases of tenotomy in which I have administered chloroform. In some of the cases which have occurred during the last two or three years, forcible movement of a stiff joint has been resorted [303/304] to, in addition to the tenotomy. I applied chloroform in St. George's Hospital in tenotomy, when the agent was first introduced; and have also given it in King's College Hospital for ten years. During these ten years I have also administered chloroform to a number of the private patients of Mr. Fergusson, whilst he has performed tenotomy, and to those of other surgeons occasionally. During the last three years, I have given it in several operations by Mr. William Adams. I understand that several orthopedic surgeons had, at one time, an objection to chloroform in tenotomy, from an impression that it would relax the muscles, and thus render the operation less easy of performance. But it is altogether unnecessary to carry the effects of chloroform so far as to relax the muscles. The pain of this operation can always be prevented without relaxing the muscles, which are indeed often more tense than if the patient were awake.
Operations for Strangulated Hernia. I have notes of only nineteen cases of operations for strangulated hernia in which I have administered chloroform since the end of 1849. This operation is, I believe, often performed without the use of this agent. Fifteen of the cases in which I have exhibited chloroform were inguinal or femoral hernia, and four cases were umbilical hernia. In these latter cases, the patients all died.
In one of the cases, there was a complication, in addition to the hernia. The patient was an old gentleman, and the surgeon had directed him to apply ice and salt, and had either given no directions respecting the time it was to be applied, or the directions were misunderstood. The patient was a scientific man, and applied the ice and salt most effectually for about four hours. When we arrived, a portion of the integuments around the umbilicus, larger than the palm of the hand, was as hard as a board, and of a dull [304/305] white colour. The surgeon said that he could not turn back the flaps of the integument, if he made them whilst it was in that hardened state. The part thawed whilst the patient was inhaling chloroform, and when the incisions were made some fluid blood of a light crimson colour flowed. Iced water was applied to the part immediately after the operation, for a short time. The integuments which had been frozen sloughed two days after the operation. The patient had peritonitis, and died on the fifth day.
On March 6th, 1848, a man was placed on the operating table in St. George's Hospital, with a strangulated femoral hernia. I administered chloroform to him at the request of Mr. H. C. Johnson; and when he became completely insensible and the muscular system relaxed, Mr. Johnson readily reduced the hernia by means of the taxis, although it was previously quite incapable of reduction. If the taxis had not been successful, the operation, for which the instruments were arranged ready, would at once have been performed whilst the patient was insensible. I do not think that chloroform has been sufficiently employed of late years during the application of the taxis to strangulated hernia.
In every case in which sickness was present, it was relieved by the chloroform. And vomiting returned in scarcely any instance, after the chloroform, so long as I remained in the room.
Operations for Hæmorrhoids and Prolapsus Ani. I have memoranda of 171 operations for these affections in which I have administered chloroform. A great number of these operations have been performed by Mr. Fergusson and Mr. Salmon; but I have also assisted Mr. Cæsar Hawkins, Mr. Bowman, Mr. Quain, Mr. Erichsen, and a number of other surgeons, whilst performing this operation. The patient always lies on one or the other side during this opera-[305/306]tion, with the knees drawn up towards the stomach. The chloroform should be inhaled till the patient is quite insensible, that is, till the edge of the eyelid can be touched without causing winking, otherwise he is apt to stretch out his legs, as soon as the operation is commenced. Ligatures always, or nearly always, introduced with a needle, have been applied to the mucous membrane in every case both of hæmorrhoids and prolapsus ani, except in two or three in which Mr. Henry Lee applied nitric acid and the actual cautery. In a great number of the cases, however, folds of redundant and diseased skin were cut away from around the anus, with a pair of large curved scissors, after the ligatures had been applied to the mucous membrane. It is the rule in these cases never to cut the mucous membrane, and never to tie the skin. It is desirable to get the patient to protrude the hæmorrhoids by bearing down at the night stool before he inhales the chloroform, and they always remain protruded during the operation; indeed, there is generally a good deal of bearing down during the operation under chloroform, and if the bowels have not been entirely emptied, they are apt to act as the operation is being performed. It is customary, and very desirable, to give a full dose of opium almost as soon as the patient wakes from the chloroform, to diminish the pain caused by the ligatures. I have, in a few cases, continued to administer the chloroform at intervals for an hour or two after the operation, till the opium began to take effect; and I consider that it would be useful, in some cases, to give the opiate two or three hours before the operation. I administered chloroform to two ladies, one a patient of Mr. Bowman, and the other of Mr. Wm. Adams, whilst hæmorrhoids were removed by the écraseur. The operations lasted rather more than half an hour; but the chloroform, after the commencement of the operation, required only to be kept up to a moderate [306/307] extent. There was no hæmorrhage in either case; and it seemed to me that the great pain which is caused by the presence of the ligatures would be prevented by this means of operating.
Hæmorrhoids and prolapsus ani are peculiarly prevalent in the upper class of society. That small portion of English people who dine in the evening seem to furnish more cases of hæmorrhoids for operation than all the rest of the population. And I am inclined to attribute the circumstance to the habit of taking the greater part of the food towards the close of the day, after a long fast; by which means congestion of the liver, and obstruction to the return of blood from the bowels is induced. Many of the patients with hæmorrhoids are ladies who are far from luxurious in their habits, indeed many of them are abstemious; and many of the male patients are the reverse of sedentary, as they spend a great part of their time in hunting, and other field sports. Again, the complaint cannot in my opinion be attributed to highly seasoned food, as I think the working classes use more pepper than fashionable people. I am inclined to believe that the habit of taking the chief meal of the day at twelve or one o'clock, is the principal reason why bad cases of hæmorrhoids are comparatively so rare in the working and middle classes, many of whom live luxuriously, and are more sedentary in their habits than the higher class of society.
Several of the patients operated on for hæmorrhoids were extremely blanched, from the continued loss of blood arising from the disease; but these patients underwent both the action of the chloroform and the operation very well. The operation, it must be remembered, is not attended with loss of blood.
Fissure of the Anus. I have notes of forty-four cases in which I have exhibited chloroform in operations for the cure [307/308] of this disease. Two of them were performed by the late Mr. Copeland. The sphincter ani was divided in the greater number of the operations. In addition to these cases, there were some in which fissure existed, along with hæmorrhoids, or fistula in ano. The patient was always placed on his side, in the same position as in the operation for hæmorrhoids.
Operations for Fistula in Ano. The position of the patient in this operation should be the same as in those for hæmorrhoids and fissure of the anus, unless the patient is placed on the back, in the lithotomy position, as I have seen in a few cases.
I have memoranda of 218 cases in which I have given chloroform in operations for fistula in ano. In many of the cases the sinuses were very numerous and extensive. It is necessary that the patient should be quite insensible during this operation, to prevent the possibility of his moving suddenly whilst the bistoury is being used.
Operations on Ovarian Tumours. I have notes of three cases in which I gave chloroform during the removal of an ovarian cyst. The first of these was in March 1850. Twenty-four pints of liquid were first evacuated from the tumour. It consisted of four cysts united together, two of which contained serous fluid of slightly different colour; the third contained serum tinged with blood, and the fourth and smallest cyst, a purulent fluid. An incision was made, twelve or fourteen inches in length, extending from the pubes to midway between the umbilicus and sternum. Some slender adhesions were removed at one spot. The tumour was attached by a membranous pedicle, with the left iliac fossa, and the fundus of the uterus. Needles were passed through the pedicle, and it was tied in three or four portions, when the tumour was removed. After the tumour was removed, the patient seemed to breathe entirely by the [308/309] ribs, the diaphragm remaining relaxed, and not contracting, whilst the wound in the abdomen was being closed. Scarcely any blood was lost during the operation. The patient died of peritonitis early on the fourth day.
The next case occurred on August 27th, 1850, and is reported in the Medico-Chirurgical Transactions for 1851. Mr. Duffin was the operator, and the patient made a favourable recovery.
The third operation was performed on the 31st of January, 1854. The patient was a spinster, twenty-eight years of age, and the tumour had not been tapped. It contained about two gallons of clear fluid, and was removed through an opening in the median line above the umbilicus, about seven inches in length. There was no depression when the patient awoke after the operation. She died within three days.
I administered chloroform in two cases where it was intended to remove an ovarian cyst. In one case the cyst was so adherent to the peritoneum that it could not be removed; in the other case, there was no cyst, but some serum in the peritoneal cavity, and a tumour growing from the fundus of the uterus. This tumour was allowed to remain. Several medical men, in addition to the operator, had diagnosed an ovarian tumour in this case. These two patients recovered.
I exhibited chloroform in four operations in which an ovarian cyst was opened, and the cut edges of it sewed to the wound in the abdominal parietes. These four patients, I believe, all died. I am quite certain as regards three of them.
On March 10th, 1852, I administered chloroform in St. Mary's Hospital to a woman, apparently about thirty-five, who had suffered from an ovarian cyst about eighteen years. Mr. Isaac Baker Brown made an incision, about six inches [309/310] in length, into the peritoneal cavity, drew out a portion of the cyst, tapped it, and removed several pints of clear serum. He then cut away a piece of the anterior wall of the cyst, about as large as the hand, and allowed the rest of the cyst to remain loose in the abdomen. The wound in the parietes of the abdomen was stitched up. If I remember rightly, the patient died, but I have no note of the result.
Operations for Cancer of the Vagina. I have notes of eighteen cases in which I have given chloroform for operations of this kind by the knife, which would have been extremely painful without the use of an anæsthetic.
I exhibited this agent, in 1848, to a lady, whilst the late Mr. Aston Key applied the actual cautery to malignant excrescence of the os uteri; and I have administered it in several cases in which potassa and other caustics have been applied to the os uteri. In operations on the vagina or perineum, the woman should inhale chloroform whilst lying on her back; and when insensible, should be drawn to the edge of the bed, or the foot of the operating table, and have the knees held back and separated.
Operations for Rupture of the Perineum. I have notes of fourteen operations for this accident. Six of them were performed by Mr. I. B. Brown, five by Mr. Fergusson, and the others by Mr. Paget, Dr. Protheroe Smith, and Mr. Henry Lee. Mr. Fergusson has, in five cases, performed an operation for prolapsus uteri, by paring the edges of the outlet of the vagina, and stitching them together so as to diminish the orifice.
I have given chloroform in several operations for vesico-vaginal fistula, some of which were performed by Mr. Spencer Wells; and also for the removal of warts and other growths from the labia pudendi, either by the knife or caustics.
Removal of the Testicle; Amputation of the Penis, etc. I have memoranda of twenty-seven cases in which I have ad-[310/311]ministered chloroform during the removal of a testicle, generally for malignant disease; and six cases in which I have administered it for amputation of the penis, always for malignant disease. There were six operations, also, in which a part of the penis was removed for malignant disease; and eleven cases in which warts were removed from the glans penis, generally with the knife. In two cases in August 1854, Mr. Acton destroyed a number of venereal warts on the glans penis and prepuce by a caustic composed of potassa and lime. In all the operations on the testicle and penis, under chloroform, the patients have been lying on the back.
Operations for Phymosis. I have memoranda of 76 operations for phymosis, in which I have exhibited chloroform. The operations were generally in the adult, although the complaint was, in most cases, congenital. I have known two cases in which cancer of the penis was produced by the patient's suffering a congenital phymosis to remain to about the age of fifty. The cancer commenced in the glans from the irritation of the retained urine. One of the patients died of the disease.
Removal of enlarged Bursa. I have notes of six cases in which the bursa of the patella was dissected out by the surgeons of King's College Hospital for housemaid's knee. The patients were charwomen and domestic servants. In two cases a bursa was removed from the forefinger.
Evulsion of the Nails. I have notes of twenty-five cases in which I have given chloroform for cutting down the nail of the great toe, and tearing away the whole, or the two edges of it; and also of three cases in which one or more finger-nails were removed by a similar process. This operation is one of the most painful of the minor operations of surgery. It is better that the patient should be lying when it is done under chloroform. [311/312]
Laryngotomy. I administered chloroform to one or two infants in which Mr. Henry Smith performed laryngotomy for croup. I also administered it, on four occasions, to a patient of Mr. Partridge, a boy four years old, who was believed to have a button in some part of the air-passages. The larynx had been opened a few days previously to the first occasion in which I gave chloroform, and I administered it on a sponge, held near to the tube in the larynx. It was necessary to give the vapour gently at first, just as if it was entering in the usual way. When it was given at all strong, whilst the patient was still conscious, he showed exactly the distress that a patient experiences when he says that the vapour produces a choking feeling; which confirms my opinion that the feeling referred to the throat, from the action of pungent vapours and gases, is caused by their presence in the lungs. The chloroform was given to keep the child quiet whilst Mr. Partridge searched for the supposed button in the larynx and bronchi. When the child recovered from the chloroform, before the operation was concluded, the explorations in its air-passages embarrassed the breathing much more, and caused more apparent threatening of suffocation, than they did when he was under the influence of the vapour. This little boy remained for months in King's College Hospital; and at last the embarrassment in his breathing subsided, the tube was removed from the larynx, and the wound allowed to heal; and he left quite well, although the button, which was supposed to have gone down his windpipe at the moment when his symptoms first suddenly came on, was never found.
I have administered chloroform in a great variety of surgical operations, in addition to those mentioned above, but as they required only the usual management in the application of the vapour, I need not allude to them, but shall, however, make a few remarks regarding dental operations. [312/313]
Extraction of Teeth. It is the custom in the medical journals and medical societies, to object occasionally to the use of chloroform in tooth-drawing, as if the operation were not sufficiently severe to require it. I will say nothing of the wives and daughters of medical men in connexion with this subject, but will only allude to the case of an elderly lady, who had for thirty years been the private friend, as well as the patient, of one of the Council of the College of Surgeons. After she had had ten necrosed teeth extracted, and had awakened from the effects of the chloroform, her friend and surgeon, who had been looking on, discoursed eloquently on her case, explaining how the state of her mouth was ruining her health; how impossible it would have been for her to go through the operation without chloroform, and what a great advantage it was.
Dr. Watson says in his Lectures:133 "I am not at all sure that the increased longevity of modern generations is not, in some degree, attributable to the capability of chewing their food which the skill of the dentist prolongs to persons far advanced in life." I have seen at least fifty cases in which the dentist has been able to exert his skill in enabling his patient to masticate only by the aid of chloroform; cases of feeble, aged, or debilitated persons, those mouths contained between twenty and thirty stumps of teeth or necrosed teeth; and who were able to get rid of them all at two or three operations a few days apart; but without the opportunity of being made insensible, would undoubtedly have continued with the mouth in a tender and painful state.
It was in consequence of the relief afforded by nitrous oxide gas, in pain caused by a tooth, that Sir Humphrey Davy suggested its application in surgical operations; it was for the extraction of a tooth that Mr. Horace Wells first carried out the suggestion of Davy; and it was in the [313/314] extraction of teeth that Dr. Morton first employed sulphuric ether as a substitute for nitrous oxide gas. These circumstances seem to point to a demand for anæsthetics in operations on the teeth; and when the great frequency of these operations is considered, it is probable that more pain may be prevented during their performance than in any other class of operations.
I have notes of 867 cases in which I have administered chloroform during the extraction of teeth, chiefly by dentists living in this neighbourhood: amongst whom are Mr. Saunders, Mr. Cartwright, Mr. Samuel Cartwright, Mr. Arnold Rogers, Mr. Thomas A. Rogers, Mr. Tomes, Mr. Bigg, Mr. Crampten, Mr. F. W. Rogers, Mr. Alfred Canton, Mr. Woodhouse, Mr. Lintott, Mr. Rahn, Mr. Vasey, Mr. Sercombe, Mr. Fletcher, and several others; and there is one dentist in the City, Mr. West of Broad Street, whom I have frequently assisted. The number of teeth, or stumps of teeth, extracted in these 867 operations, has been about 3021. In some cases in which several teeth have been removed, I have not been sure of the exact number, but have put down about the number.
The number of teeth extracted at an operation has varied from one to nineteen. The latter number was extracted by Mr. Canton on one occasion, and on two or three occasions, Mr. Arnold Rogers and Mr. Samuel Cartwright extracted seventeen at one sitting; but these gentlemen and others, as well as myself, have thought it better, as a general rule, to make more than one operation, when the number of teeth to be drawn exceeded ten, in order that the mouth might not contain too many wounds at one time, and that the loss of blood might not be very great. A great number of the operations have been for the extraction of the four first permanent molars, in children about thirteen, as these teeth are very apt to decay at an early period. [314/315]
I have on 181 occasions, of which I have memoranda, given chloroform for the extraction of a single tooth. I exhibited it lately to a lady, aged eighty-six, whilst Mr. Bigg extracted an abortive wisdom tooth, which had recently come through the gum, and was giving pain. She awoke in about two minutes after the operation, and was quite cheerful and well.
The patients have been seated in an easy chair in all the operations on the teeth, except in a very few cases where a female patient was too ill to sit up. In many cases, and always if there was any feeling of faintness, the patient has been placed on a sofa, after the operation, for twenty minutes or half an hour. I am not aware of any inconvenience from the chloroform, in any of the cases of tooth-drawing, excepting sickness and vomiting, which in a very few of the cases have been troublesome for some time.
It is necessary in tooth-drawing to make the patient unconscious, and to continue the chloroform a little while after unconsciousness is induced, till the sensibility of the edge of the eyelid is very much diminished, or almost altogether suspended, otherwise the patient will probably make a resistance that will interfere with the operation, or scream out and alarm his or her friends. I nearly always take about four minutes in the inhalation. It is not desirable to take longer than five or six minutes, as the patient would be slower than is desirable in recovering completely from the effects of the vapour.
The patient is usually in the third degree of narcotism when the operation is performed, and, in this degree, as was previously stated, there is not unfrequently a contracted and rigid state of the muscles. This state often affects the muscles of the jaws, and interferes with the opening of the mouth, if it be closed. I generally tell the patient to keep his mouth open whilst inhaling, and by that [315/316] means it often remains open when he is insensible. Not unfrequently, however, he closes it on becoming insensible. One can generally open it by pressing on the chin; but as the chin does not afford a very favourable hold, there are a very few cases in which the mouth cannot be opened easily in this way, at least not unless the effects of the chloroform are carried further than is desirable for these operations. I therefore carry with me a little instrument of two blades, made to open by means of a screw. The ends of the blades are covered with leather, and, if introduced between the teeth, at the corner of the mouth on the side opposite to that on which the dentist is about to operate, the mouth can easily be opened.134 The power of the instrument is only such that I can scarcely open it with one hand, when I hold the blades with the other. It would not enable one to open the mouth of an adult if he were closing it by voluntary power; but the spasm caused by chloroform is very much less powerful than the action of the muscles when influenced by the will. I never use the instrument for opening the mouth when the patient is closing it voluntarily under the influence of a disordered, consciousness, but always wait till consciousness and volition are entirely suspended. When the mouth is once opened, it can generally be kept open with the fingers, and the instrument may be withdrawn.
The bleeding during tooth-drawing is never so free as to interfere with the breathing; but when more than two or three teeth are extracted, and especially if they be in the back part of the mouth, some of the blood which escapes nearly always flows into the stomach; it flows down the fauces and œsophagus usually without any act of deglutition; but the evidence of its having gone into the stomach is obtained in those cases where the patient vomits. In [316/317] consequence of the blood flowing into the stomach, vomiting cannot so generally be prevented by the precaution of not taking a meal before the operation in tooth-drawing as in other operations; but the sickness usually subsides as soon as the patient has emptied his stomach.
The chloroform has occasionally to be repeated in tooth-drawing before the operation is completed, especially in cases where several teeth require to be extracted. When this is the case, I always reapply it as soon as the patient begins to show signs of feeling the operation, without waiting till he recovers his consciousness. In many cases, however, a number of teeth are extracted without any repetition of the chloroform; and in the instances in which as many as fifteen, seventeen, or nineteen teeth were extracted at one operation, it was chiefly because the first application of the vapour enabled the dentist to take out such a number, otherwise, in most of these cases, a number of the teeth would have been left for a succeeding operation. It has occasionally happened, however, that the chloroform has required to be repeated, once or twice even, for the extraction of a single stump. When the chloroform is repeated once or twice, it is generally a longer time before the patient is able to leave the dentist's house. I always request the patients who are operated on at the dentist's, to drive home, as it is not advisable to walk, or use any exertion for an hour or two after the action of chloroform. Indeed, the patient is usually disinclined for any exertion for twenty minutes or half an hour after the influence of this agent, and sometimes for much longer; although I have seen a patient mount the box of a sort of dog-cart, and drive himself away, within five minutes after having several teeth extracted whilst he was in a state of complete insensibility from chloroform.
I have administered chloroform in a great number of [317/318] cases for the destruction of the nerves of the teeth. The patient requires to be made as insensible in this operation as in tooth-drawing.
Secondary Hæmorrhage after Operations. The hæmorrhage which occasionally comes on several days after an operation, from sloughing, ulceration, or the non-formation of a coagulum in an artery, is probably as liable to occur now as formerly; but I believe that hæmorrhage, a few hours after an operation, is much less frequent since the practice of narcotism by inhalation. Before this practice, it was extremely common for the patient to faint during an operation, when the bleeding of the smaller arteries stopped, and they escaped the ligature, to break out in hæmorrhage occasionally afterwards; but under the influence of narcotic vapours it is unusual for the patient to faint, and consequently every vessel which is capable of bleeding is tied during the operation.
When the practice of inhalation in midwifery was first introduced by Dr. Simpson, he very naturally adopted the plan which is usually followed in surgical operations, making the patient unconscious at once, and keeping her so to the end of the labour. It was soon found, however, by other practitioners, that this is not necessary; and, indeed, it would not be safe in protracted cases. Drs. Murphy and Rigby were, I believe, amongst the first to state, that relief from pain may often be afforded in obstetric cases, without removing the consciousness of the patient; and I soon observed the same circumstance.135 Some persons, indeed, have alleged that the pain of labour can always be prevented, without making the patient unconscious of surrounding objects; whilst others have asserted that no relief can be [318/319] afforded unless unconsciousness be induced. But both these opinions are directly opposed to experience. There are comparatively few cases in which the suffering can be prevented throughout the labour without interfering with consciousness, although there are very many cases in which it can be in this way prevented in the early part of the labour. This difference depends, in some measure, on the constitution of the patient, but chiefly on the severity of the pain to be prevented. It is in accordance with what is observed in medical and surgical cases, that the pain should be removed, in some instances, without abolishing consciousness, and that in other instances it should not; for, in certain cases of neuralgia, the pain is so severe, that no material relief can be obtained by chloroform as long as consciousness is retained; and in surgical operations, although it now and then happens that the minor and concluding parts of an operation, such as tying vessels and introducing sutures, can be performed without pain, whilst the patient is consciously looking on, a free incision in the skin can hardly ever be made, under similar circumstances, without pain.
With regard to the cases of labour in which chloroform may be employed, it will be readily conceded that, in cases where the pain is not greater than the patient is willing to bear cheerfully, there is no occasion to use chloroform; but when the patient is anxious to be spared the pain, I can see no valid objection to the use of this agent, even in the most favourable cases. The benefits arising from chloroform in severe cases of labour are experienced in a lesser degree in favourable cases; and the patient may be fairly allowed to have a voice in this, as in other matters of detail which do not involve the chief results of the case. The determination of the kind of labours in which chloroform should be used, or withheld, is really a matter of not much importance, because, as we pass from cases that are severe and [319/320] protracted to those which are short and easy, the quantity of chloroform that is used, and the amount of diminution of the common sensibility, and of interference with the mental functions, become so trifling, that very little remains about which to hold a discussion. Indeed, from what I have observed of the continued use of this agent in medical cases, and its use by healthy persons for experiment, I believe that the quantity which is inhaled in a short and easy labour might be continued daily for an indefinite period, without appreciable effect on the health.
The above remarks apply also, in some measure, to the question as to the period of the labour when the exhibition of chloroform should commence; for, in proportion as the pains are feeble, it must be more sparingly administered. The most usual time when the accoucheur and I have determined that the inhalation should be commenced, has been when the os uteri was nearly dilated to its full extent, and the pains were taking on an expulsive character. In many of the cases which I have attended, it has, however, been commenced much earlier; for the suffering caused by the dilating pains in the first stage of labour is often very great, and the chloroform is consequently of the utmost service when employed at this time.
As regards the manner of giving chloroform, I shall first allude to cases not requiring manual or instrumental assistance. In such cases, when it has been determined to resort to inhalation, the moment to begin is at the commencement of a pain; and the chloroform should be intermitted when the uterine contraction subsides, or sooner, if the patient is relieved of her suffering. It is desirable to give the chloroform very gently at first, increasing the quantity a little with each pain, if the patient is not relieved. The practitioner easily finds, with a little attention, the quantity of vapour which it is desirable to give at [320/321] any stage of the labour, and in each particular case; his object being to relieve the patient without diminishing the strength of the uterine contractions and the auxiliary action of the respiratory muscles, or with diminishing it as little as possible. At first, it is generally necessary to repeat the chloroform at the beginning of each "pain"; but, after a little time, it commonly happens that sufficient effect has been produced to get the patient over one or two uterine contractions without suffering, before it is resumed.
The external evidences of the uterine contractions continue as before, when the patient is rendered unconscious by chloroform; and the muscles of respiration are called freely into play, to assist the action of the uterus in the second stage of labour. The aspect of the patient under these circumstances, is generally that of one who is suppressing the expression of her sufferings; and any relative or friend who comes in, without knowing that chloroform has been given, begins to praise the unconscious patient for her fortitude. On some occasions, indeed, there are groans and cries, as of suffering; but the mind being unconscious of pain, it can hardly be said to exist.
It may be remarked, that complete anæsthesia is never induced in midwifery, unless in some cases of operative delivery. The diminution of common sensibility to a certain extent, together with the diminution or removal of consciousness, suffice to prevent the suffering of the patient during labour; and she never requires to be rendered so insensible as in a surgical operation, when the knife may be used without causing a flinch or a cry. The nerves of common sensation must be allowed to retain their functions to a certain extent during labour; otherwise the assistance of the respiratory muscles, which consists of reflex action, or "motion arising from sensation, without the aid of voli-[321/322]tion", would not take place, even if the contractions of the uterus should still continue.
The effects of chloroform on the brain should not be carried during labour beyond what I denominate the second degree of narcotism, or that condition in which the mental functions are diminished, but not altogether suspended, except when the effect of the vapour is associated with natural sleep. The patient under the influence of chloroform to this extent, has no longer a correct consciousness of where she is, and what is occurring around her, but is capable of being aroused to give incoherent answers, if injudiciously questioned. In this state, the patient will sometimes assist the labour by bearing down voluntarily, if requested to do so, and be otherwise obedient to what is said; and by withholding the chloroform for a few minutes, she at any time becomes quite conscious. As a general rule, it is desirable not to hold any conversation whilst the patient is taking chloroform, in order that her mind may not be excited. The plan mentioned above, of giving the chloroform very gently at first, also has a tendency to prevent its causing mental excitement, the patient coming gradually under its effects. In surgical operations, excitement of the mind can nearly always be avoided by carrying the patient pretty rapidly into a state of insensibility, in which the mental functions are necessarily suspended. But in the practice of midwifery, it is not allowable to cause a state of coma or insensibility, except in certain cases of operative delivery, hereafter to be mentioned.
I nearly always employ, in obstetric cases, the inhaler that I use in surgical operations. There is not the same necessity for an accurate means of regulating the proportion of vapour in the air which the patient is breathing during labour, where but a trifling amount of narcotism requires to be induced, as in surgical operations, where a deeper [322/323] effect is necessary; still I find the inhaler much more convenient of application than a handkerchief, and it contains a supply of chloroform which lasts for some time, thereby saving the trouble of constantly pouring out more. When I do administer chloroform on a handkerchief during parturition, I follow the plan of putting only ten or fifteen minims of chloroform on the handkerchief at one time.
The quantity of chloroform administered during any one pain, never exceeds a very few minims; but the quantity used in the course of a protracted labour is often considerable. I have several times used from four to six ounces; and in one case, at which I was present the greater part of the time, seventeen fluid ounces of chloroform were used with the inhaler, which would produce as much effect as three or four pounds used on a handkerchief. The inhalation was continued with intermissions over a period of thirty-one hours. The patient was unconscious during the greater part of the last five or six hours, but previously to this, her constant complaint was that she had not enough chloroform. She was the wife of a physician, was thirty-seven years of age, and in her first confinement. The membranes ruptured early. The labour was natural, but there was excessive sensibility. The first twenty-six hours of intermitted inhalation were during the first stage of labour.
Chloroform can be best applied when there is an additional medical man, who has not to attend to the ordinary duties of the accoucheur; but it can be given very well by the accoucheur himself, so as to save the greater part of the suffering of labour; although he perhaps cannot always administer it in the perfect way in which he could, if he had no other duties to divide his attention.
It is probable that the use of chloroform has no particular influence over the duration of labour, in the whole number of cases in which it is employed; but individual [323/324] labours are occasionally either retarded or quickened by it, according to circumstances. In some cases, the chloroform, even when very moderately employed, diminishes both the strength and the duration of the uterine contractions, and prolongs the interval between them, thereby making the labour somewhat longer--a matter of no consequence, however, as the patient is not suffering in any way. In other cases, the inhalation causes the uterine action to become stronger and more regular, by removing the excess of sensibility by which it has been interfered with. This occurs more particularly in the first stage of labour. In some cases, also, the chloroform seems to act as a direct stimulant to the uterine contractions, increasing their force and frequency--a circumstance at which we need not be surprised, when we remember that both opium and brandy, in moderate quantity, often act in the same manner. Chloroform has also the effect of promoting the dilatation of the os uteri in many cases, even when no rigidity exists; and when there is rigidity of the os uteri, the inhalation is of the utmost service, and shortens labour very much. This is the case, also, when there is rigidity of the perineum.
When the forceps have to be applied, it is desirable to make the patient insensible, as if for a surgical operation just before they are applied; and to leave off the chloroform as soon as they are introduced, in order to allow of the uterine action to return, and assist in the delivery. I have always found the action of the uterus return immediately after the forceps were introduced; and where the child was not delivered at once, I have continued the chloroform in sufficient quantity to keep the patient unconscious, whilst allowing the uterine contractions to continue.
I have administered chloroform on nine occasions in which the forceps were applied; in four of the cases, I was sent for in consequence of the operation being required; [324/325] and in the other five cases, I was in attendance from an early part of the labour, and had administered chloroform more or less for some hours before the forceps were applied. They were applied in three instances by Dr. Murphy, twice by Dr. Ramsbotham, and in the other cases by Drs. Farre, Frere, and Thudichum, and Mr. Peter Marshall.
I have administered chloroform in two cases of craniotomy, both of which were performed by Dr. Murphy, on account of deformity of the pelvis. The amount of chloroform scarcely requires to be increased during this operation beyond what would be given according to the strength of the pains which may be present at the time.
In the operation of turning the child, the mother requires to be made quite insensible, in order that the uterine contraction may be entirely suspended till the legs of the child are brought down, when the inhalation should be discontinued to allow the contraction of the uterus to return. I have notes of six cases of turning the child, in which I have administered chloroform. The first case, which occurred in 1848, was one of natural presentation, in which turning was performed by Dr. Murphy, on account of narrowness of the pelvis, and the impossibility of applying the forceps; the introduction of the hand was difficult on account of want of space, but the uterus offered no resistance. Dr. Murphy has related the case. Three of the other instances of turning were performed by Mr. French, in cases which had been attended by midwives, and the membranes had been ruptured for several hours. The shoulder and part of the chest were in each case pressed down into the pelvis, and the pains were very strong; yet under a full chirurgical dose of chloroform, the child was turned as easily as if the membranes had not been ruptured. In the first of these three cases, the child was dead before the operation commenced. In the other two, it was born alive. In the [325/326] last case, the membranes had been ruptured for ten hours before the operation was performed. After the child was delivered, there was found to be a second child presenting naturally, but I did not stay to give any more chloroform. The fifth case of turning was performed in a case of elbow presentation by Mr. Peter Marshall. The membranes had been previously ruptured. I administered chloroform, also for Mr. Marshall, in a case where the hand was presenting below the head; he raised it above the head, and as it did not come down again when the pains returned, the labour was allowed to pursue its natural course, and terminated favourably in two or three hours, the child being alive. The chloroform was not continued after the operation was performed. The remaining case of turning was performed by Mr. Tegart, of Jermyn Street. I was in attendance with him from an early stage in the labour, and the operation was performed before the membranes were ruptured.
I administered chloroform, in 1849, in a case in which Dr. Murphy had to make an artificial os uteri. The patient was, of course, made quite insensible as for any other surgical operation; and the vapour was continued afterwards in a modified degree till the labour was completed.
On December 26th, 1850, I was requested by Mr. Cooper, of Moor Street, Soho, to assist him in a case of retention of the placenta. The patient had given birth to a child two hours before, and Mr. Cooper had introduced his hand, but had been unable to bring away the placenta, on account of firm contraction of the uterus in a sort of hour-glass form. On the chloroform being administered, the hand was easily introduced, and the placenta detached, and extracted. There was very little hæmorrhage.
In some of the many cases at which I have met Dr. Cape, premature labour was induced about the eighth month of utero-gestation, by rupturing the membranes, on account of deformity of the pelvis. [326/327]
In a case attended by Mr. Cantis, the patient was suffering from osteo-sarcoma of the bones about the shoulder. Dr. Ferguson was present during the latter part of the labour. The lady lived a few weeks after her confinement.
A patient, attended in her confinement by Mr. Colambell of Lambeth, in 1853, to whom I gave chloroform, had been long under the care of Dr. Williams with cavities in the lungs. I heard very lately that she was still living.
A patient of Mr. Robert Dunn, to whom I gave chloroform in her confinement, was at the time in a state of insanity.
In one of the patients whom I have attended with Dr. Arthur Farre, there was separation of the recti muscles of the abdomen; which there is no doubt must have taken place gradually during pregnancy. The patient was but twenty years of age, and in her first labour. Quite early in the labour, before the pains were at all strong, Dr. Farre and I observed that the abdomen was of a peculiar form, the uterus projecting very much forwards, whilst there was a slackness in the flanks. The abdominal muscles did not assist the pains at all; and it was probably from this cause that the labour progressed slowly and was terminated at last with the forceps. The recti muscles recovered their position by careful bandaging.
The chloroform has always been left off as soon as the child was born, but a little has been administered again on several occasions during the expulsion of the placenta. The placenta has generally been expelled very soon in the labours in which I have given chloroform; usually in about five minutes. There has hardly ever been uterine hæmorrhage of any amount, except in patients who had suffered from it in previous labours. In a case attended by Mr. Nathaniel Ward, however, there was a slight hæmorrhage before the birth of the child, and about an hour afterwards [327/328] there was a considerable hæmorrhage which made the patient feel rather faint for some hours. She afterwards went on favourably, however. She was a young woman who had had several children.
A patient, to whom I was recommended by Sir John Forbes, inhaled chloroform in three confinements. She recovered favourably from the two first; but on the third occasion, after going on favourably till the fifth day, she was attacked with puerperal fever, and died on the seventh day from her confinement.
I am not aware that more than one death has been recorded as having occurred from chloroform during labour; and this took place in England, in 1855, when no medical man was present.136 The patient had inhaled chloroform in America in a previous labour; but her medical man, on the last occasion, who was her particular friend, forbad that agent, and said that if she was determined to have it, he would not attend her. She procured chloroform unknown to him, and a number of scents to put on her handkerchief and hide the odour of it from him. He went to bed in the house, and was not called up till his patient had been dead about an hour. The monthly nurse, who had procured the chloroform for the patient, said that she snored very loudly for an hour after she fell asleep. About five drachms of chloroform were used from the bottle, and the handkerchief from which it was inhaled remained close to the patient's face till she died. The death seemed to have taken place very slowly, and the monthly nurse was extremely stupid to allow the patient to die. It may also be remarked that the accident would not have taken place except for the medical man's extreme objection to the use of chloroform.
The chloroform has been occasionally blamed by the [328/329] friends of patients, or medical men opposed to its use, in cases where patients have died from puerperal convulsions or other causes, so long after the vapour had been left off that it could not be the cause of death. The following case shows how easy it would be to make a mistake with respect to the effects of chloroform. Soon after its introduction, I was requested to administer it to the wife of a medical man who had a great desire for it in her confinement. Mr. Propert was to attend the lady. I was sent for late one evening, but as there were no pains at the time when I arrived, I was requested to go to bed in the house. After a time, I was called by a servant, who told me that the baby was born, and that Mr. Propert was sent for. I found that the birth had been so sudden that the husband, who was in the room, could not get to the bed side before the child was born. Mr. Propert arrived, and I went home, leaving the patient very well. Mr. Propert informed me, that after I left the patient went into such a state of syncope as to make him think she was going to die, and continued so for some time. She ultimately recovered. There was no hæmorrhage or any other cause to account for the faintness, and I understood Mr. Propert to say, that if the patient had inhaled chloroform, he should have blamed it for the condition into which she lapsed.
Neuralgia. When the pain of neuralgia is not extremely severe, it may be removed by the inhalation of chloroform without causing unconsciousness; but when it is very severe, it is necessary to make the patient unconscious before the pain is suspended. In some cases of neuralgia of the face, the pain is so severe that the signs of it remain after the patient is rendered unconscious, and only disappear when he is quite insensible; and then, as the insensibility [329/330] passes off, the hand is raised to the face, and the contortions of the features return before the patient awakes to be aware of his suffering. When the mental branch of the fifth nerve is affected, the paroxysms of pain are accompanied by a motion and smacking of the lips. In a hospital patient I have seen this when he was awake, but in a gentleman only when his consciousness was removed by the chloroform, and before complete insensibility was induced; when awake, he restrained the impulse to this kind of motion of the lips.
In administering chloroform it is desirable to continue it steadily and gradually till the pain is relieved; and if the patient is rendered unconscious before the pain is removed, to continue it till all signs of suffering disappear. After the first inhalation of the vapour, the pain will generally return in a few minutes, but when again subdued, it will not return so quickly; and after it has been suspended a few times by the repetition of the chloroform during the space of an hour or so, the pain is usually removed either permanently or for two or three hours. In some cases I have had to repeat the chloroform occasionally throughout the day, and, on one or two occasions, for two or three days in succession. The chloroform can, in general, only be considered a temporary remedy, and therefore such other medicines should be applied as may be thought advisable.
When I have prescribed chloroform in a liniment, to be applied to the face, the patient has often found out that he obtained more relief by smelling at the liniment than by applying it. Chloroform generally gives great relief, however, when applied locally in neuralgia, either alone or mixed with camphorated spirit; it is advisable to apply it on a piece of lint or blotting paper, which should be covered over with tinfoil, or some other impermeable substance, to prevent the evaporation. It causes about as much heat and [330/331] uneasiness as a mustard poultice, before it relieves the pain.
Spasmodic Asthma. On November 12th, 1850, I administered chloroform in the Hospital for Consumption, at Brompton, to a married woman, aged thirty-five, a patient of Dr. Cursham. She was in a fit of spasmodic asthma, but was the subject also of chronic bronchitis. Twenty minims of chloroform were inhaled from an inhaler. It gave immediate relief, producing a momentary state of unconsciousness, or a state bordering on it. In a few minutes the difficulty of breathing gradually returned, but not to the same extent, and the inhalation was repeated with a like effect. The difficulty of breathing returned less quickly and severely; and after a third inhalation of twenty minims she was completely relieved, and could lie down. The patient had a good night, and was better next day. On the 14th, she had another fit of spasmodic asthma, which was relieved completely by the chloroform in the same manner as the previous one. This patient inhaled extract of stramonium every evening, by a method which will be described further on.
Other cases of spasmodic asthma have been relieved as readily and completely; but in one or two cases, in which the difficulty of breathing seemed to depend on disease of the heart, the relief was not so great; the patient went to sleep, but the breathing remained embarrassed.
Spasmodic Croup. I have administered chloroform in seven cases of this complaint. It was recommended in every instance by Dr. Ferguson, and all the cases ended in recovery. The children were from eight months to two years of age; the majority being about a year. I always gave enough chloroform to cause a state of unconsciousness, for which a few minims suffices in a young child, and when the effect passed off, or nearly so, I repeated the dose. I [331/332] generally gave five or six doses in the course of about half an hour, after which the child would often sleep for two or three hours. In the milder cases it was repeated once a day; but in the more severe cases it was continued, in the above manner, twice a day. I administered it to a patient of Dr. Van Oven, respecting whom Dr. Ferguson had been consulted, for fifteen days, twice every day, excepting the last three days. This child was very ill when the treatment was first commenced, having a severe fit of spasmodic breathing every five minutes. When the chloroform is given during the spasm, it is desirable to give it very cautiously.
Mr. W. J. H. Cox read a paper on the treatment of laryngismus stridulus, with chloroform, at the London Medical Society, in 1850. He had entrusted the administration of it to the mother or nurse, and directed it to be given whenever the spasmodic breathing should come on. I am inclined to think that this would be the best way of giving it, if one could be quite sure of the intelligence of the party to whom it was intrusted.
Hooping Cough. I have only administered chloroform in two cases of this complaint. It was recommended in both cases by Dr. Ferguson. One of the children was extremely ill of bronchitis, and it died. The other child recovered, but the chloroform was not continued. I am not aware that chloroform has had any fair trial in hooping-cough. It should be given whenever a fit of coughing comes on.
Infantile Convulsions. I have administered chloroform in two cases of this disease, with the effect of relieving the convulsions, but the children died. They were both extremely ill before the chloroform was administered. One was the patient of Mr. Walter Bryant, and Dr. Seth Thompson was consulted about it. A case has been related by Dr. Simpson of Edinburgh, in which the chloroform was [332/333] continued for a day or two, and in which the infant recovered.
Delirium cum Tremore.137 Some cases have been related in the medical journals, in which this complaint was treated successfully by chloroform alone; but I prefer to use this agent only as an adjunct to the treatment by opium. Sometimes the patient is so violent and suspicious that he cannot be made to take opium; but it is much easier to make a person breathe a medicine, than swallow one. It is only necessary to hold a patient, and to apply the chloroform near his face, and he is obliged to breathe it, and as the effect of it subsides, he recovers the power of swallowing before his delirium returns; for whilst he is still unconscious, he will swallow whatever is poured into his throat. Opium can be administered, and the chloroform can be repeated occasionally so as to keep him asleep for an hour or two till the opium takes effect and prolongs the sleep. It is a great advantage of chloroform that the delirium may be subdued in a few minutes by it, and can be kept away till opium takes effect.
In certain cases of delirium cum tremore, such a quantity of opium is taken without procuring sleep, that the medical attendant has, what I believe to be, a well-grounded fear of giving more. A patient whom I saw with Mr. Peter Marshall, in April 1850, had taken ten fluid drachms of laudanum and two grains of acetate of morphia, within twenty-four hours of my seeing him, without any sleep being [333/334] procured. He was put to sleep immediately by chloroform, which was repeated on the following day. The patient got quite well in a few days.
In December 1851, I saw a patient who had had no sleep for four days, except three intervals of a quarter of an hour each, although a great deal of opium had been given. He was very violent; and for the last twelve hours had spat out all the medicine that was given to him; his pulse was small and very rapid. He was made insensible in a few minutes, and the chloroform was repeated, at intervals, for half an hour, so as to keep him unconscious. Fifty minims of tincture of opium were given in one of the intervals. I waited an hour and a quarter after the chloroform was discontinued; the patient was still sleeping, and his pulse was less frequent. I learnt that when he awoke he was quite free from delirium, and he was well in a few days.
Delirium in Fever. In November 1857, I administered chloroform to a youth of seventeen, who had been ill of typhoid fever for sixteen days. He had been in a state of constant delirium for upwards of forty-eight hours without having the least sleep, although he had had tincture of opium in divided doses to the extent of forty-five minims, and had taken a tablespoonful of wine every four hours. The chloroform was continued gently for half an hour; he slept for an hour afterwards, and at intervals during the night. He was a little better in the morning; and the delirium was not again so violent as it had been. He died on the nineteenth day of the fever, from a recurrence of diarrhœa.
Dr. Fairbrother, of Bristol, gave small doses of chloroform by inhalation, with the best effects, in a case of typhus fever, in the Bristol Infirmary. The patient was delirious and worn out for want of sleep, her life being in fact de-[334/335]spaired of. She inhaled the chloroform occasionally for several days, sleep being always procured when it was applied, and she recovered without any other medicine.138
Hydrocephalus. I administered chloroform on two occasions, for half an hour at a time, to a child, seven years old, when delirious and screaming violently, in this complaint. The child was much relieved by the inhalation, but it died on the fourteenth day of the disease.
Tetanus. I have notes of three cases of tetanus in which I have administered chloroform. The first was a patient of the late Mr. Keate, in St. George's Hospital, in February 1849. It was a girl, fourteen years old, who had received some severe burns in the face and various parts of the body, a fortnight previously. Four days before inhaling the chloroform, she was attacked with symptoms resembling those of chorea, but for the last two days the complaint was recognised to be tetanus. There was rigidity of the spine and jaws, and of one arm, which was flexed. Spasms came on every minute or two, affecting, more particularly, the head and the arm. I commenced to give chloroform very gently at four in the afternoon. It prevented the spasm before consciousness was quite removed. Whenever the spasm offered to return, the inhalation was repeated with the effect of stopping it. The chloroform was continued till half-past five, with the effect of keeping the spasm away; and the patient took some drink during this time, better than she had done previously. I saw the child again at eight o'clock in the evening, and found that the spasms had returned soon after I left, and had continued as before. The chloroform was given again at intervals for an hour and a half, with the effect of keeping away the spasms, and inducing sleep; but I found that the child was getting [33/336] weaker, and would die even if the spasm was entirely prevented. She died at a quarter past eight the following morning. There was no inspection of the body.
The next case was a patient of Mr. Propert, a boy, ten years of age, who had suffered from sloughing of the skin of the inferior extremities. The tetanus came on during the healing process, whilst the greater part of both extremities was in a state of ulceration, and covered with healthy granulations. The patient was in a very irritable and feeble state, and his pulse was 150 in the minute. He was made insensible, and the chloroform was repeated twice in the space of half an hour. No relaxation of the muscles of the jaws was produced, although the effect of the chloroform was carried as far as seemed safe in such a subject. He died twelve hours afterwards.
I administered chloroform lately to a patient of Mr. Salmon in St. Mark's Hospital. He underwent an operation by ligature for prolapsus ani and hæmorrhoids on March 1st; on March 5th tetanus commenced, and on March 7th chloroform was administered whilst Mr. Salmon removed some sloughs from the anus; and it was repeated occasionally afterwards. The patient was a man, fifty-two years of age; he was the subject of kidney disease, and the tetanus was extremely severe. He had had four doses, each containing a fluid drachm of laudanum, between the time when the tetanus commenced and his inhaling the chloroform. His pupils were contracted, and he was made insensible by an extremely small quantity of chloroform. He was, in fact, very much under the influence of opium, although the spasm of the tetanus prevented his sleeping.
Chloroform affords great relief to the patient affected with tetanus, and it probably increases the prospect of recovery in cases which are not too severe and acute.
Epilepsy. Dr. Todd at one time had chloroform admi-[336/337]nistered by inhalation, in King's College Hospital, to the extent of causing insensibility, at stated intervals, in cases of epilepsy, and he thought with advantage. I have frequently administered chloroform for surgical operations to patients who were subject to epilepsy, and have very rarely found it produce any approach to a fit.
In July 1850, I administered chloroform to a boy, seven years old, in an epileptic fit, which had lasted about an hour when the inhalation was commenced. He had had fits previously, the last of which had occurred a year before, but none of them had lasted so long as the existing one. He had eaten nine new potatoes for his dinner, at one o'clock, and the fit came on about eight. I found the abdomen swollen and very tympanitic. There was constant convulsive motion of the right arm, and of the neck; the latter drawing the head to the right side. The mouth was also drawn to the right at each convulsive motion. The chloroform was given by putting a few minims at a time on a handkerchief, and holding it to the mouth and nostrils. It caused immediate cessation of the convulsions every time it was applied. The convulsions, however, returned again in a minute or two. In the intervals that he was partially under the influence of the vapour, he breathed easily without stertor. The convulsions became gradually less severe, and ceased entirely ten or fifteen minutes after the commencement of the inhalation.
Puerperal Convulsions. I have not been called to any case of this complaint since chloroform has been in use; but some cases have been related in the medical journals in which the inhalation of chloroform has been employed with a favourable result. One case is related by Mr. Henry Rudge, of Leominster.139 When the chloroform was admi-[337/338]nistered, the patient was in violent convulsions which came on in frequently succeeding fits. The os uteri was dilated, and the head presenting. The pains were entirely arrested. The chloroform was administered by twenty minims, at intervals, on a folded handkerchief. The convulsions, after a few inhalations, entirely ceased, and Mr. Rudge extracted the child without difficulty. There was another child with the head presenting: it was delivered with the forceps. The placenta was delivered with the hand on account of smart hæmorrhage. There was only one attack of convulsions after delivery, and the patient recovered favourably. It was her first labour, and her age was twenty-three years.
A case of puerperal convulsions was related by Mr. Andrew Bolton to the Newcastle and Gateshead Pathological Society.140 His patient, aged twenty-two, was at the full period of her first pregnancy. The os uteri was high, slightly dilated, and extremely rigid. She was treated at first by bloodletting, and full doses of morphia. Mr. Bolton says: "As her condition appeared hopeless should the paroxysms continue, chloroform was administered on a piece of linen, in half-drachm doses, and its full effects kept up for three hours. At two P.M., there was a slight return of convulsion; skin warm and perspiring; the os uteri was found steadily dilating; and from her uneasy movements, it was apparent that uterine action had begun.
"Half-past three. The membranes were ruptured; and brisk uterine action ensuing, a dead child was expelled, immediately followed by the placenta. She regained her senses during the expulsive efforts, but appeared entirely ignorant of her previous condition. Recovery followed without any bad symptom.
"In conclusion, I would remark, that the convulsions were in no measure mitigated by the depletion, which was [338/339] carried to the utmost; nor was there any yielding of the os uteri until the chloroform was inhaled."
The urine was not examined in either of the above cases, and it is not stated that œdema was present.
Hysterical Paralysis and Contractions. In December 1851, I administered chloroform in Charing Cross Hospital to a young woman about twenty-five, a patient of Dr. Chowne. She kept her left knee in a semiflexed position, and would not allow it to be moved. She had been in bed in the hospital for two months. She inhaled the chloroform reluctantly, and, after becoming unconscious, she breathed and sobbed in a hysterical manner. When insensible, the limb went down flat on the bed, the knee being quite movable. A straight splint was applied, and the limb was secured to it with bandages. I was informed that in a few days she contrived to get her leg bent again. She was the domestic servant of a nobleman. It was evident that there was nothing the matter with her limb, and that it was only influenced by her volition, which was perverted by the hysteria under which she was labouring.
In November, in the same year, I administered chloroform in the same hospital to another patient of Dr. Chowne, whose case was more obscure and complicated. The patient was a woman, aged thirty-three, who represented that for several months she had been unable to open her mouth, or to speak, and that she had, for the same length of time, been paralyzed in the left arm and leg. The affection, it was said, came on suddenly, in a kind of fit, which was followed by unconsciousness for three or four weeks. It was also said, that she had one or two fits the previous year, after which she was unconscious for a long time. The patient was quite conscious before inhaling the chloroform, and replied to questions by nodding or shaking the head, or by writing on a slate. She was unmarried, and had not [339/340] menstruated for some months past. The chloroform was administered with a view to ascertain whether or not she was feigning. On first becoming unconscious, the patient breathed in a sobbing and hysterical manner. The chloroform was given very gradually; and as she became more affected, there were some struggling and rigidity, when the right arm and leg were moved about a good deal. The left arm and leg were also distinctly moved, but not above a tenth part as much as the extremities of the opposite side. When the patient was quite insensible, the limbs being relaxed, the pupils turned upwards, and the conjunctiva insensible, attention was turned to the jaws, which were still firmly closed, but they were opened by using a moderate degree of force with the fingers. The effect of the chloroform having been allowed in a great measure to subside, it was again administered, when the movements of the limbs recurred, and there was the same difference between the motion of the right side and that of the left, as before. When I left the patient, more than half an hour after the chloroform was discontinued, she had not opened her eyes or answered questions; and she did not do either for six days. I saw her five days after the chloroform. The pulse was very rapid on my first going to the bedside, but its frequency subsided in a few minutes. On my raising the eyelid, she turned her eye about, as if endeavouring to hide the pupil under the lid. On the following day she answered questions by nodding and writing on a slate, and was, in other respects, the same as before inhaling the chloroform.
The great difference in the amount of motion in the limbs of this patient, under the influence of chloroform, showed that the paralysis of the left side was not a mere pretence. It is, indeed, possible that the absence of motion in the limbs of the left side, for several months, would cause them [340/341] to move less than the opposite ones during the action of chloroform; but it is not to be supposed that the patient would keep these limbs in one posture during the night, and when no one was present, without ever moving them, unless she herself believed that they were paralyzed. I looked on the woman as a sick person, and not a mere impostor; for although she appeared to exaggerate her symptoms, and to have a good deal of pretence and affectation, this circumstance arose, no doubt, from her complaint.
In April 1853, I administered chloroform four times to a patient of Dr. Arthur Farre, a girl of fifteen years of age, who was affected with a contraction of the flexor muscles of the left thigh and leg, of the muscles which bend the body to the left side, and those which bend and turn the head to the same side, in consequence of which the leg was drawn up, and the body and head were curved greatly to the left side. The contraction of the muscles had lasted for several weeks, but she had been ill for a much longer period, her illness having commenced with a fever. She took an extremely small quantity of nourishment, and was very thin. Her bowels were moved with difficulty. The pulse was very feeble and small, and there was a tendency to coldness of the surface. An eminent surgeon in the provinces had expressed his opinion that the distortion of the limbs and trunk was a feigned disorder; but the action of the chloroform proved that he was altogether in error. The muscles became completely relaxed when the patient was quite insensible, and the limbs and trunk and head could be readily moved into any position; but as the effects of the chloroform subsided, the deformity returned on each occasion before the patient recovered her consciousness. Neither the chloroform nor any other measures were of any service, and Dr. Farre informed me that the patient died a few weeks after I saw her. [341/342]
Mania. I have been informed of several cases in which chloroform has been administered in acute mania, with the effect of calming the patient and procuring sleep. I have administered it in two cases with the same temporary advantage. In one of the cases, the patient was persuaded to inhale it; in the other, he had to be held by three keepers till he was unconscious. An eminent and well-known scientific man, who became insane some years ago, refused to take food. It was found that after being made unconscious by chloroform, he would take a meal just as he recovered from its effects, and the chloroform was given before every meal for a long time.
Spasmodic Pain. In August 1851, I administered chloroform to a woman who was labouring under a severe paroxysm of spasmodic pain in the abdomen. The pain was completely removed, without altogether causing unconsciousness. An opiate was given to prevent the pain from returning.
I have not had the opportunity of administering chloroform during the passage of calculi down the ureters, or of gall-stones; but there can be no doubt that it would be of the greatest service in such cases. If Dr. Griffin had been provided with chloroform when he attended the late Mr. Augustus Stafford with an attack of gall-stones,141 he would have been able to relieve his patient in five minutes, instead of taking two or three hours to produce relief by opium. There would have been no occasion for the venesection, which was carried to thirty ounces. And at the end of the attack, on Dr. Griffin leaving his patient for the night, if chloroform had been employed, he would have left him without any appreciable amount of the narcotic in his system. As it was, however, he left him with a quantity of opium unabsorbed from the alimentary canal. The bandage [342/343] got displaced from the arm; there was an additional hœmorrhage, the opium became absorbed more quickly, and a dangerous state of narcotism was induced.
Frequent and long-continued Use of Chloroform. Many patients have inhaled this agent hundreds of times, and it continued to produce insensibility as readily as at first. The dose does not require to be increased on account of its long use. I was informed of the case of a lady who was affected with a painful cancer, and was attended by the late Mr. Keate and Mr. Henry Charles Johnson. She inhaled chloroform at frequent intervals, by day and night, for a very long time, consuming three or four ounces in the twenty-four hours.
In November 1851, a surgeon in the north of England wrote to me respecting one of his patients, a lady, who had inhaled a great deal of chloroform, on account of neuralgia of the uterus. He said that, during that year, and principally within the last six months, she had inhaled at least two hundred ounces; that she often inhaled as much as three ounces in a day; and that it seemed to have produced very little effect on her general health, except that she seemed to be more susceptible of pain. He said that he had reluctantly yielded to the entreaties of his patient to administer it so often, and he wished for my opinion respecting the propriety of continuing its use, and what effect it would be likely to produce.
I advised that the chloroform should be continued as long as the severity of the pain rendered it necessary; and expressed my opinion, that it would produce as little ultimate effect as any other narcotic which might be used to relieve the pain. I saw the surgeon in September of the following year. He informed me that the chloroform was continued for some time after he had written to me; but [343/344] that his patient had recovered from her complaint, and had left off the chloroform, and was in good health.
Mr. Garner, of Stoke-upon-Trent, has related the case of a lady, affected with neuralgia, who inhaled sixty-two ounces of chloroform from her handkerchief, in twelve days.142
History and Composition. "This liquid is first described by Valerius Cordus, in 1540, under the name of oleum vitrioli dulce. The term ether was applied to it a hundred and ninety years afterwards by Frobenius, who, in a paper in the Philosophical Transactions, described its singular properties; at the end of this paper is a note by Godfrey Hankwitz, Mr. Boyle's operator, mentioning the experiments that had been made upon it by Boyle and by Newton."143
The present chemical name of ether, or sulphuric ether, is oxide of ethyle. It consists of four atoms carbon, five atoms hydrogen, and one atom oxygen. Its atomic number is consequently 37.
The usual way of making ether, is to distil common alcohol (the hydrated oxide of ethyle) with sulphuric acid.
Chemical and physical Properties. Ether is a clear, colourless liquid, of the specific gravity of 0.715 at 68°. It boils at 96° Fahr.; and the specific gravity of its vapour is 2.565. It is soluble, in all proportions, in alcohol, and it is soluble in nine parts, by measure, of water. Water is also soluble in nine parts, by measure, of ether, so that after ether has been agitated with water, it retains one-tenth of its volume of that fluid. Ether is very inflammable, and, as it yields its vapour very freely, great care is required in pouring it out by artificial light. Its vapour is also very explosive when mixed, in certain proportions, with atmospheric air. [345/346]
The ordinary ether of the shops contains a portion of alcohol which has distilled over with it; the alcohol should be removed by agitating the ether with twice its volume of water, before it is used for inhalation. The ether which has been treated in this way is called washed ether. The water which it takes up during the washing can be removed by distilling it from lime, or dry carbonate of potassa; but this is unnecessary, as the water does not interfere with the action of the ether when inhaled; and part of the water evaporates and is inhaled with the ether, when the atmospheric air is not already saturated with moisture.
Ether has a peculiar and very strong odour; in this respect it differs extremely from chloroform. The odour of a single drop of ether can be distinctly perceived all over a large operating theatre, whilst a pint of chloroform may be spilt without its odour being much noticed. The strong odour of ether is, indeed, one of the greatest objections to its use, since another agent has been discovered which is free from this objection. As was previously stated, the odour of chloroform cannot be perceived in the breath, after the lungs are emptied by one or two expirations of the vapour just taken in; whilst the smell of ether can be perceived in the breath for twenty-four, and sometimes for forty-eight, hours after the patient has inhaled it. The surgeon, and others who have been about the patient, also smell of the ether to a less degree. When a rabbit has been killed by the inhalation of ether, a starving cat will not eat its flesh even after it has been boiled; whereas the odour of chloroform cannot be perceived in the bodies of animals that have been killed by it.
If ether is exposed to atmospheric air by being kept a long time in a bottle but partly filled, it is apt to be decomposed into acetic acid and water. [346/347]
The following Table shows the result of experiments which I made to ascertain the quantity of vapour of ether that 100 cubic inches of air will take up, when saturated with it, at various temperatures, the barometric pressure being 30 inches of mercury. The ether I employed in the experiments was washed, but not dried. It was, therefore, saturated with water, of which it contained one-tenth of its volume. It had a specific gravity of 0.735 at 60° Fahr., and it boiled at 98°.

In the above Table the air is a constant quantity of 100 cubic inches, which becomes expanded to 152, and so on; but the following Table shows the quantity of vapour in 100 cubic inches of the saturated mixture of vapour and air at different temperatures:--

[347/348]

The absorption of caloric during the evaporation of ether is much greater than during that of chloroform, owing both to the greater quantity of vapour it yields on account of its lower boiling point, and to the lower specific gravity of the vapour. The evaporation of ether from the bulb of a thermometer usually lowers the temperature nearly to zero of Fahrenheit. When the inhalation of ether was first commenced, the inhalers employed consisted generally of glass vases containing sponge, to afford a surface for the evaporation of the ether. Both glass and sponge being very indifferent conductors of caloric, the interior of the inhalers became much reduced in temperature, the evaporation of ether was very much checked, and the patient breathed air much colder than the freezing point of water, and containing very little of the vapour of ether. On this account, and through other defects in the inhalers, the patient was often very long in becoming insensible, and, in not a few cases, he did not become affected beyond a degree of excitement and inebriety.
To ensure the ether taking effect in a short time in every case, I made use of the conducting power of the metals, and the great capacity of water for caloric. The inhaler [348/349] which I employed was made of plated copper, and was placed in two or three pints of water, of the ordinary temperature. The form of the inhaler was that of one which had been contrived by Mr. Julius Jeffries for the inhalation of aqueous vapour.144 No sponge or bibulous paper, or other material, was used; and the air, before being inhaled, was made to pass over a considerable surface of ether by means of a spiral volute, soldered to the top of the inhaler, and reaching nearly to the bottom. The accompanying engraving shows the interior of the inhaler, on a scale of half the dimensions, the bottom being removed.
The Physiological Effects of Ether are essentially the same as those of chloroform. The various degrees of narcotism which I described in the earlier part of this work, when treating of chloroform, were first described by me when treating of ether in 1847, before chloroform was in use.145 All the remarks which I made with respect to the [349/350] manner in which age, strength or debility, and other circumstances, influence the action of chloroform, apply also in an equal degree to ether.
I performed some experiments in 1848,146 for ascertaining the proportions of vapour of ether present in the blood in the different degrees of narcotism. They were conducted on the same principles as those previously related, which were performed for the purpose of determining the same point in regard to chloroform.
Experiment 31. Two grains of ether were put into a jar holding 200 cubic inches, and the vapour diffused equally, when a tame mouse was introduced, and allowed to remain a quarter of an hour, but it was not appreciably affected.
Experiment 32. Another mouse was placed in the same jar, with three grains of ether, being a grain and a half to each 100 cubic inches. In a minute and a half, it was unable to stand, but continued to move its limbs occasionally. It remained eight minutes without becoming further affected. When taken out, it was sensible to pinching, but fell over on its side in attempting to walk. In a minute and a half, the effect of the ether appeared to have gone off entirely.
Experiment 33. A white mouse in the same jar, with four grains of ether, was unable to stand at the end of a minute, and at the end of another minute ceased to move, but continued to breathe naturally, and was taken out at the end of five minutes. It moved on being pinched, began to attempt to walk at the end of a minute, and in two minutes more seemed quite recovered.
Experiment 34. Five grains of ether, being two and a half grains to each 100 cubic inches, were diffused throughout the same jar, and a mouse put in. It became rather more quickly insensible than the one in the last experiment. [350/351] It was allowed to remain eight minutes. It moved its foot a very little when pinched, and recovered in the course of four minutes.
Experiment 35. A white mouse was placed in the same jar with six grains of ether. In a minute and a half, it was lying insensible. At the end of three minutes, the breathing became laborious, and accompanied by a kind of stertor. It continued in this state till taken out, at the end of seven minutes, when it was found to be totally insensible to pinching. The breathing improved at the end of a minute; it began to move at the end of three minutes; and five minutes after its removal, it had recovered.
Experiment 36. The same mouse was put into this jar on the following day, with seven grains of ether, being 3.5 grains to the 100 cubic inches. Stertorous breathing came on sooner than before; it seemed at the point of death when four minutes had elapsed; and being then taken out, was longer in recovering than after the last experiment.
Experiment 37. Two or three days afterwards, the same mouse was placed in the jar, with eight grains of ether, being four grains for each 100 cubic inches. It became insensible in half a minute. In two minutes and a half, the breathing became difficult; and at a little more than three minutes, it appeared that the breathing was about to cease, and the mouse was taken out. In a minute or two, the breathing improved; and in the course of five minutes from its removal, it had recovered.
The temperature of the mice employed in the above experiments was about 100°. That of the birds in the following experiments was higher, as is stated; and they differ widely from the mice in the strength of vapour required to produce a given effect, although I found but little difference between the mice and birds, in this respect, in the former experiments on chloroform. And one of the linnets was [351/352] employed in both sets of experiments. Having seen MM. Dumeril and Demarquay's statement of the diminution of animal temperature from inhalation of ether and chloroform, before the following experiments were performed, the thermometer was applied at the beginning and conclusion of some of them. I have selected every fourth experiment from a larger series on birds.
Experiment 38. 18.4 Grains of ether were diffused through a jar holding 920 cubic inches, being two grains to each 100 cubic inches, and a green linnet was introduced. After two or three minutes it staggered somewhat, and in a few minutes more appeared so drowsy, that it had a difficulty in holding up its head. It was taken out at the end of a quarter of an hour, quite sensible, and in a minute or two, was able to get on its perch. The temperature under the wing was 110° before the experiment began, and the same at the conclusion.
Experiment 39. Another linnet was placed in the same jar, with four grains of ether to each 100 cubic inches of air. In two minutes it was unable to stand, and in a minute more, voluntary motion had ceased. It lay breathing quietly till taken out, at the end of a quarter of an hour. It moved its foot slightly when it was pinched. In three minutes it began to recover voluntary motion, and was soon well. The temperature was 110° under the wing, when put into the jar, and 105° when taken out.
Experiment 40. A green linnet was put into the same jar with 55.2 grains of ether, being six grains to 100 cubic inches. It was insensible in a minute and a half, and lay motionless, breathing naturally, till taken out at the end of a quarter of an hour. It moved its toes very slightly when they were pinched with the forceps, and it began to recover voluntary motion in two or three minutes. Temperature 110° before the experiment, and 102° at the end. [352/353]
Experiment 41. A linnet was placed in the same jar, containing eight grains of ether to each 100 cubic inches. Voluntary motion ceased at the end of a minute. The breathing was natural for some time, but afterwards became feeble, and at the end of four minutes appeared to have ceased; and the bird was taken out, when it was found to be breathing very gently. It was totally insensible to pinching. The breathing improved, and it recovered in four minutes.
Experiment 42. 9.2 grains of ether, being one grain to each 100 cubic inches of air, were diffused through the jar, holding 920 cubic inches of air, and a frog was introduced. At the end of a quarter of an hour, it had ceased to move spontaneously, but could be made to move its limbs, by inclining the jar so as to turn it over. At the end of half an hour, voluntary motion could no longer be excited, and the breathing was slow. It was removed, at the end of three-quarters of an hour, quite insensible, and the respiratory movements being performed only at long intervals, but the heart beating naturally; and it recovered in the course of half an hour. The temperature of the room was 55° at the time of this experiment.
We find from the 32nd experiment, that a grain and a half of ether for each 100 cubic inches of air, is sufficient to induce the second degree of narcotism in the mouse; and a grain and a half of ether make 1.9 cubic inch of vapour, of specific gravity 2.586. Now the ether I employed boiled at 96°. At this temperature, consequently, its vapour would exclude the air entirely; and ether vapour, in contact with the liquid giving it off, could only be raised to 100° by such a pressure as would cause the boiling point of the ether to rise to that temperature. That pressure would be equal to 32.4 inches of mercury, or 2.4 inches above the usual barometrical pressure; and the vapour [353/354] would be condensed somewhat, so that the space of 100 cubic inches would contain what would be equivalent to 108 cubic inches at the usual pressure. This is the quantity, then, with which we have to compare 1.9 cubic inch, in order to ascertain the degree of saturation of the space in the air-cells of the lungs, and also of the blood; and by calculation, as when treating of chloroform,
So that we find 0.0175, or 1-57th to be the amount of saturation of the blood by ether necessary to produce the second degree of narcotism; and as by Experiment 35, three grains in 100 cubic inches produced the fourth degree of narcotism, we get 0.035, or 1-28th, as the amount of saturation of the blood in this degree. Now this is within the smallest fraction of what was found to be the extent of saturation of the blood by chloroform, requisite to produce narcotism to the same degrees. But the respective amount of the two medicines in the blood differs widely; for whilst chloroform required about 288 parts of serum to dissolve it, I find that 100 parts of serum dissolve five parts of ether at 100°; consequently 0.05 x 0.0175 gives 0.000875, or one part in 1142, as the proportion in the blood in the second degree of narcotism; and 0.05 x 0.035 gives 0.00175, or one part in 572, as the proportion in the fourth degree.
In Experiment 42 the frog was rendered completely insensible by vapour of a strength which was not sufficient to produce any appreciable effect on the mouse in Experiment 31. This is in accordance with what was met with in the experiments with chloroform. Air, when saturated with ether at 55°, contains 32 grains in each 100 cubic inches; so that the blood of the frog might contain 1-32nd part as much as it would dissolve, which, although not quite so great a proportion as was considered the average for the fourth degree of narcotism in the mice, yet was more [354/355] than sufficient to render insensible the mouse in Experiment 34.
There is a remarkable difference between the birds and the mice, in respect to the proportions of ether and air required to render them insensible, a difference that was not observed with respect to chloroform. In some experiments with ether on guinea-pigs, which are not adduced, they were found to agree with mice in the effects of various quantities.
The birds were found to require nearly twice as much; five grains to 100 cubic inches, the quantity used in an experiment between the thirty-ninth and fortieth, which is not related, may be taken as the average for the fourth degree of narcotism in these birds, with a temperature of 110°. By the kind of calculation made before, we should get a higher amount of saturation of the blood than for the same degree in mice. But as serum at 110° dissolves much less ether than at 100°, the quantity of this medicine in the blood of birds is not greater than in that of other animals; and, considered in relation to what the blood would dissolve at 100°, the degree of saturation is the same.
By Experiments 36, 37, and 41, we find that with ether, as with chloroform, a quantity of vapour in the air, somewhat greater than suffices to induce complete narcotism, has the effect of arresting the respiratory movements.
In treating of chloroform (page 74), the average quantity of serum in the adult human subject was estimated at 410 fluidounces [sic]. In order to find the quantity of ether in the system, we may multiply 410 by 0.000875 for the second degree of narcotism, and by 0.00175 for the fourth degree, when we shall obtain 0.358 and 0.71 of an ounce, i.e. f. ʒii. ɱl [2 fluid drachms + 50 minims] in the first instance, and f. ʒv. ɱxl [5 fluid drachms + 40 minims] in the second. In the third degree of narcotism, in which surgical operations are usually performed, the quantity is intermediate, or a little over four drachms.
On the Administration of Ether. About a fluid ounce of ether is usually inhaled by an adult patient in becoming insensible; fully one-half of this is, however, thrown back from the lungs, windpipe, nostrils, and face-piece, without being absorbed. I usually put two fluid ounces of ether into the inhaler above described, at the beginning of the inhalation, and this quantity often lasts to the end of the operation, if it is not a protracted one. The inhaler is connected, by means of a wide elastic tube, with a face-piece similar to that described and delineated in treating of chloroform. It is necessary that the inhalation should commence, as in the case of chloroform, with the expiratory valve of the face-piece turned on one side, for the admission of air which is not charged with ether, and that the vapour should be admitted to the air-passages by degrees, to avoid the irritation that would arise from suddenly inspiring any considerable quantity of the vapour. The vapour of ether is very much less pungent than an equal quantity of the vapour of chloroform; but as the patient requires to breathe about six times as much of it in the inspired air, it feels quite as pungent as that of chloroform, and, perhaps, a little more so. Whilst the patient never requires to take in more than four or five per cent of vapour of chloroform in the inspired air, he requires to inhale about thirty per cent of vapour of ether, in order to be rendered insensible in a convenient time. The air-passages, however, soon get accustomed to the presence of the vapour of ether, and in a minute and a half or two minutes after the patient begins to inhale, he can usually bear the valve to be closed so far as to charge the air with as much vapour as is necessary speedily to cause insensibility. The inhaler yields quite sufficient vapour when the water-bath is at 50° Fahr.; and at the seasons of the year when the temperature of the water is higher, the expiratory valve of the face-piece can be left more or less open to ad-[356/357]mit a portion of air which has not passed through the inhaler.
I prefer the flavour of ether vapour to that of chloroform; and the sensations I experience from the inhalation of ether are more pleasurable than those from chloroform. Many persons agree with me on both those points; but some prefer chloroform. The quantity of ether expended in causing insensibility is eight or ten times as great as that of chloroform, but the quantity used in a protracted operation is not so disproportionate; for, owing to the great solubility of ether and the large quantity of it which is absorbed, it is much longer in exhaling by the breath, and when the patient is once fairly insensible, it does not require to be repeated so frequently as chloroform.
In administering ether, I usually rendered adult patients insensible in four or five minutes, and children in two or three minutes. A somewhat longer time was occasionally occupied in cases in which the air passages were irritable, or where there was much rigidity and struggling. I never failed to make the patient insensible in any one instance in which I administered ether. I have notes of 152 cases in which I administered ether, before chloroform was introduced, and twelve cases in which I have exhibited it since.
Nearly all the great operations of surgery were included several times amongst the cases in which I administered ether. Amputation of the thigh was performed in nineteen cases; fifteen of the patients recovered, and four died. Amputation of the leg was performed eleven times; eight of the patients recovered, and three died. The arm was amputated three times; one of the patients died, and two recovered. There were thus thirty-three of the larger amputations with eight deaths, being a mortality of twenty-four per cent. There were two amputations of the forearm, and both patients recovered. There were nine operations of [357/358] lithotomy; seven of the patients recovered, and two died. Five of the patients were children, who all recovered; the two deaths occurring amongst the four adult patients. Eighteen female patients had the breast removed for tumour, and they all recovered except one.
On July 1st, 1847, Mr. Cutler amputated the leg of a man, aged forty-four, in St. George's Hospital, who had suffered from disease of the tibia and ankle, which had existed thirty years, and was caused by an accident. This patient died on the seventh day, of sloughing phagedena, which was present in the hospital. It was then found that he had disease of the heart. Its structure was soft and easily lacerable; much fat was mixed up with the muscular structure. The aortic valves were much thickened, and almost cartilaginous in structure. Two of them were so much contracted that they were together about the size of a healthy one. The left ventricle was dilated, and the right ventricle still more so; its walls being extremely thin. The ether had acted quite favourably on this man.
I administered ether repeatedly in infants and old people. Some of the infants were operated on by Mr. George Pollock, in 1847, for congenital cataract by drilling; and two of them were operated on, in 1857, for hare-lip, by Mr. Ferguson and Mr. Bowman. A gentleman, one of whose toes the late Mr. Liston amputated in 1847, was said to be subject to apoplectic attacks. The ether acted very favourably. Amongst the operations which Mr. Liston performed on patients to whom I administered ether, was the tying of the external iliac artery in a man, aged forty, for an aneurism of the groin, situated partly above Poupart's ligament. The patient lay perfectly still in this, as in all the other important operations in which I administered ether. He recovered.
On June 18th, 1847, I exhibited, in University College [358/359] Hospital, ether to a man, aged forty-two, with stricture of the urethra, caused by an accident. He passed his urine only in drops, and the attempts to pass a catheter had all failed. It was Mr. Liston's intention to divide the urethra in the perinæum, but when the patient was placed fully under the influence of ether to the fourth degree of narcotism, a catheter (No. 1) passed into the bladder, and the operation was not required. Larger catheters were introduced in a few days, and on July 27th, the patient was discharged, being able to pass his urine in a good stream.
Ether was administered in many cases of midwifery by Dr. Simpson, who had first applied it in obstetric cases, and by a number of other practitioners. I only exhibited it in one case, and then only for a short time. Mr. Lansdown of Bristol used it in thirty cases.147 In one case, it was continued for eleven hours and a half, and fourteen fluid ounces of ether were used. He said that he invariably found the perinæum relaxed before the head came to bear on it, thereby not requiring the pressure of the head to force it open, in cases where ether was used. He says: "I find the uterus sending out the placenta immediately after the expulsion of the child, and there has been scarcely any hæmorrhage following." Mr. Lansdown said that he had found the action of the uterus to be induced by ether, when in a sluggish state, but he had not found this effect from chloroform, in the cases in which he had used it.
Ether was used with great advantage in most of the kinds of medical cases in which chloroform was afterwards applied. In the summer of 1847, an infant, nine months old, was brought to me in a convulsive fit, which had lasted twenty minutes. I poured twenty minims of ether on a sponge, and applied it to its mouth and nostrils; in two or three minutes, the quantity was repeated. The spasm sub-[359/360]sided, and the child fell asleep. It had no return of the fit. It was labouring under hooping-cough at the time, which had existed a week.
The inhalation of ether was employed in the treatment of asthma, hooping-cough, and tetanus, before it was employed in surgical operations. It has been already stated (page 14) that Dr. Richard Pearson administered the vapour of ether in consumption in 1795. Dr. Robert Willis sent an article to the Medical Gazette on February 2nd, 1847,148 in which the following passages occur.
"Ether, given by the mouth, has long been familiarly employed in the treatment of asthma. I have for many years been aware of the fact that it is vastly more efficacious, administered directly in vapour by the breath. My plan of using it is extremely simple. I have had recourse to no kind of apparatus for this purpose, but have been content to pour two, three, or four drachms of the fluid upon a clean handkerchief, and to direct this to be held closely to the mouth and nostrils: a single short and difficult inspiration is hardly made before the effect is experienced; and I have occasionally seen the paroxysm ended in six or eight minutes, the respiration having in that brief interval become almost natural.
"It is not otherwise with hooping-cough: the paroxysms of coughing are positively cut short by having the ether and the handkerchief in readiness, and using them when the fit is perceived to be coming on."
I have been informed of a case of tetanus which was treated successfully by inhalation of ether more than twenty years before this medicine was used to prevent the pain of operations, but I am not able at present to give a reference to the case. Mr. C. A. Hawkesworth, surgeon, of Burton-on-Trent, wrote me an account of a case of tetanus, which [360/361] had recovered under the inhalation of ether in 1847. The patient was a healthy-looking butcher's boy, about twelve years old, who had received a slight scalp wound, which was followed by general tetanus. Mr. Hawkesworth administered the vapour of ether to him during the greater part of one day. The spasm relaxed most completely whilst the influence of the ether continued, but returned in great degree when the inhalation was intermitted. He took no other medicine except calomel and jalap, with a view to purgation; the calomel, however, acted on his mouth. He recovered speedily and completely. Some other cases of recovery from tetanus under the inhalation of ether have been recorded in the medical journals.
In February, 1847, Dr. Sibson related several cases of facial neuralgia that had been greatly benefited by the inhalation of ether; 149 and it has been used in many cases since.
The inhalation of ether causes an increased flow of saliva in many cases; quite as frequently, in fact, as chloroform. Vomiting also follows the use of ether quite as often as that of chloroform. The insensibility from ether lasts longer than that from chloroform without repeating the inhalation when the narcotism is carried to the same degree. When the narcotism from ether is carried to the fourth degree there is generally a complete absence of pain for three minutes, and a state of unconsciousness for five minutes longer, a period during which any pain there might be would not be remembered afterwards. On account of this longer duration of the effects of ether, it is better adapted than chloroform for certain operations on the face, as removal of tumours of the jaws, the operation for hare-lip, and making a new nose. The relaxation of the muscular system from the effects of ether seems greater in general than from chloroform, and ether therefore seems to be the better agent to employ in the reduction of old dislocations, and strangulated hernia. [361/362]
Great safety of Ether. I believe that ether is altogether incapable of causing the sudden death by paralysis of the heart, which has caused the accidents which have happened during the administration of chloroform. I have not been able to kill an animal in that manner with ether, even when I have made it boil, and administered the vapour almost pure. The heart has continued to beat after the natural breathing has ceased, even when the vapour has been exhibited without air; and in all cases in which animals have been made to breathe air saturated with ether vapour, at the ordinary temperatures of this country, they have always recovered if they were withdrawn from the vapour before the breathing ceased. Even in cases where the natural breathing had ceased, if the animal made a gasping inspiration after its removal from the ether it recovered.
I hold it, therefore, to be almost impossible that a death from this agent can occur in the hands of a medical man who is applying it with ordinary intelligence and attention.
I am only aware of two deaths which have been recorded as occurring during the administration of ether, and it is not probable that the death in either case was due to the ether. The first of these cases occurred in France, at the Hotel Dieu d'Auxerre, on July 10th, 1847.150 The patient was a man fifty-five years of age, who had a cancerous tumour of the left breast of seven months duration. He was robust, and had no general lesion resulting from the cancerous disease. The ether was exhibited with the apparatus of Charrière. The patient had hardly inhaled two or three minutes when he became strongly excited. The trunk and limbs were agitated with violent starts and shocks. The breathing became frequent, and the face injected. He endeavoured to push away the inhaler, and [362/363] babbled as if drunk. This state lasted for five minutes, and the prick of a pin showed that sensibility still remained. The apparatus was still applied, but in opening to the ether vapour an issue as large as the instrument permitted; for the tap which gave passage to it had hitherto been but half turned, and that progressively. At the end of ten minutes from the beginning of inhalation, the relaxation and immobility of the limbs was complete, the insensibility was not doubtful, the respiration was deep, gentle, but free from râle. The muscles of the face had ceased to be agitated, and it was of a violet red colour, as was also the skin in front of the chest; the pupils were turned upwards, dilated and immoveable.
The apparatus was taken away, and the operation was commenced; but the incision had only given issue to a small quantity of black blood, when it was perceived that the features were altered and become entirely violet, and that the respiration was extremely feeble. The pulse, touched on this moment for the first time, was soft, full, and very slow. All at once it ceased to beat.
Twenty-four hours after death, all parts of the body yielded a strong odour of ether. The blood was deep black, fluid, and rather viscous. The blood which gorged the back part of the lungs had a consistence and colour somewhat like treacle. The mucous membrane of the bronchi, trachea, and larynx was very much congested. The spleen was so softened in its interior as to resemble the lees of wine.
This patient appears to have died rather from the want of admission of sufficient air to the lungs than from the effects of ether. The apparatus was applied without intermission, long after the face became injected, and was kept applied till it became of a violet colour. The pulse was not felt till the patient was dying. Artificial respiration [363/364] was not attempted, although it would most likely have restored the patient.
The other death which happened whilst the patient was under the influence of ether took place at the Hotel Dieu de Lyons, on September 11th, 1852.151 The patient was a woman, aged fifty-five, but looking much older. She was affected with a tumour of the superior maxillary bone, and was weak and in a bad state of general health. M. Barrier was reluctant to remove the tumour, but yielded to the entreaties of the patient. The ether was administered from a sponge placed in a bladder, and the patient was quickly put to sleep. M. Barrier had made the incisions in the face, and had just divided the ascending process of the jaw, when the breathing stopped. There was no pulse at the wrist, and it was doubtful whether there was any at the precordial region. The patient was placed horizontally, and artificial respiration and other measures were applied, but without success.
This patient evidently died of hæmorrhage; the mode of death which M. Barrier must have been dreading, as we perceive from his reluctance to perform the operation. According to the result of my experiments on animals, ether is not capable of causing the kind of death which this patient died.
There were three or four cases in which ether was blamed by the operating surgeons for causing the death of patients, who recovered from its effects, and died some days, or at least hours, afterwards. The nature and circumstances of the operation were sufficient to account for the fatal result in each of these cases, whilst the extended use of ether has confirmed the opinion that it cannot be the cause of deaths which occur days, or even hours, after its use. [364/365]
On Friday, the 12th of February, 1847, Mr. Roger Nunn performed lithotomy, in the Colchester Hospital, on a man who, as it was found after his death, had disease of the kidneys. The ether seemed to act favourably. Mr. Nunn says: "There was neither difficulty nor loss of time in cutting into the bladder; but having done so, some little delay occurred in grasping the stone, which was small, very flat, and lying in the posterior part of the bladder; the delay was also increased by the extremely relaxed state of the bladder itself, which seemed to fall in folds on the forceps, and to cover the stone."152 This delay in grasping the stone is attributed by Mr. Nunn to a collapsed state of the bladder caused by the ether, but it can only have arisen from the fact of the urine having escaped from the bladder, before the stone was seized. The small vessels divided in making the first incision showed much inclination to bleed, and Mr. Nunn secured them immediately after the patient was put to bed.
Speaking of his patient and the ether, Mr. Nunn says: "He recovered from its effects after a short time, and continued in a quiet passive state, but without decided reaction for twenty-four hours. At this period he had a chill, which lasted for nearly twenty minutes." Stimulants were given, but without much effect. The patient seemed incoherent from eight o'clock P.M. of Saturday till nine A.M. of the following day. From this time he gradually sank, and died at five o'clock P.M. of that day, Sunday, being sensible to the last.
On March 9th, 1847, Mr. Wm. Robbs, of Grantham, removed an osteo-sarcomatous tumour from the back part of the left thigh of Ann Parkinson, a married woman, aged twenty-one, the mother of one child.153 Mr. Robbs tried to make his patient insensible with ether, but did not succeed. [365/366] He says, indeed, that in about ten minutes its usual effects were produced; but these could not have been its full and proper effects; for he says, "she appeared quite sensible to the pain during the whole of the operation." It is reported that she appeared to feel the first cut. Mr. Robbs says that during the early part of the operation, the patient "cried out much, complained, and writhed in great agony of pain." The operation was begun by an incision commencing midway between the tuberosity of the ischium and the trochanter major, and extending about six inches down the thigh. The fascia was next divided, and the muscles were next separated with the handle of the scalpel, so as to expose the upper surface of the tumour. After this had been done, the inhaler was replaced to the mouth of the patient whilst the operation proceeded, but the ether appeared to take no effect. The tumour was "very adherent to the long head of the biceps flexor cruris, which nearly covered it anteriorly, while posteriorly it rested on the sheath of the great sciatic nerve. It took its origin from the common tendon of the flexor muscles, close to the tuber ischii, and was inserted into the short head of the same muscle just below its origin." Mr. Robbs says: "The dissection was protracted longer than I expected, from the violent contractions of the muscles, and the struggles of the patient." He estimated the time occupied in the operation at twenty-five or thirty minutes; and the sister-in-law of the patient, who gave her evidence at the inquest, expressed her opinion that the operation lasted an hour all but five minutes. At the end of the operation, the patient appeared very faint, and the pulse was very rapid and feeble. The patient remained much depressed, with a pulse of 140 in the minute, small, and without much power, having her intellect perfect; she died forty hours after the operation.
A coroner's inquest was held, but neither the coroner nor [366/367] any of the jury appeared to have any knowledge or suspicion that a surgical operation on the thigh could possibly be the cause of death. A surgeon who gave evidence stated, that "the shock from the operation was not simply the cause of death, as the seat of the disease was not essential to life." The verdict was, that the death of deceased was caused by the inhalation of ether; and that no blame was attached to the surgeon, as ether had been used and, recommended by eminent medical men.
I cannot tell whether Mr. Robbs would have undertaken the operation if ether had not been about to be used, but if he had undertaken it without ether, one may presume that he would have done what every surgeon does who undertakes a great operation, that he would have informed the patient and her friends that it would be attended with some amount of danger. In his communication to the Medical Gazette, Mr. Robbs complains of the friends of his patient having thought it necessary to obtain a coroner's inquest; but he has himself to blame for that. After he had attributed the death entirely to a new agent, which had been given with a view to prevent the pain, and had entirely failed even in that, it was very natural that they should seek for a legal investigation of the affair.
Mr. Robbs makes no admission that the pain his patient suffered could be due to any defect in the administration of the ether. He states, that he "was quite unprepared for that perfect state of prostration of the brain and nervous system which it appears in this case to have induced". The fact of the patient crying much, and complaining, and writhing in great agony of pain, and the contraction of the muscles, and the struggles which protracted the operation, do not look like a prostration of the brain and nervous system. At the end of the operation she was, to be sure, prostrated by its long duration, and the great loss of blood [367/368] which must have occurred; but her brain and nervous system were not so much affected as the vascular and muscular system. She spoke of the operation as having been very severe, and she retained her mental faculties perfectly to her death. Ever since 1818 many of the students at lectures on chemistry had inhaled the vapour of ether to quite as great an extent as Mr. Robbs' patient.
As a proof how far the feelings will suspend both reason and common sense, it may be mentioned that some of the medical men, who were strongly opposing the use of ether in 1847, did not hesitate to allude to the inquest in this case, as showing that ether had caused the death of a patient.
Mr. Eastment, of Wincaiton, Somersetshire, related a case154 in which he attributed the death of the patient to ether. It was apparently the first time he had seen ether employed on the human subject; and with a larger experience of its effects, he would no doubt alter his opinion respecting the cause of death in the case he related.
A boy, aged eleven years, became entangled in the machinery of a mill, about eight A.M., on February 23rd, 1847, in consequence of which he sustained a very severe compound fracture of the left thigh, with great laceration of the soft parts, and a simple fracture of the right thigh. The surgeons in attendance waited till four P.M. for the boy to recover from the shock of the injury, and then performed amputation of the left thigh. Ether was given, but so badly, that the patient's sufferings were so severe on the circular incision being made, that it appeared to be a complete failure. The inhalation was repeated, however, and the pain of the latter part of the operation was prevented. The patient died three hours after the operation, being in a state of great exhaustion, with occasional mental excitement, during the three hours. [368/369]
This patient's chance of life would probably have been improved if the ether had been more effectually given, so as to prevent all the pain of the operation; but I believe that his chance of recovery would have been most improved by administering the ether soon after the accident in the morning, which would most likely have removed the collapse, and enabled the surgeon to perform amputation at once, and thus have prevented the eight hours suffering and depressing effects of the great laceration of the thigh.
M. Bouisson155 has mentioned a case in which death was attributed to ether by a surgeon named Roël, of Madrid. Dolorès Lopes, aged fifty, of very feeble constitution, and addicted to drunkenness, had long suffered from a cancerous tumour of the breast. It was removed after the patient had inhaled ether for half an hour, and it weighed three pounds and a quarter. The patient died seven hours after the operation. But the operation itself was sufficient to account for the death of such a patient; and she could not die from ether at the end of seven hours after inhaling it.
On account of its great safety, ether is extremely well adapted for medical cases, in which it is necessary that a narcotic vapour should be administered by the patient's nurse.
The Combination of Chloroform and Ether. Some practitioners have recommended the inhalation of the vapour from a mixture of chloroform and ether; but the result is a combination of the undesirable qualities of both agents, without any compensating advantage. Ether is about six times as volatile as chloroform--that is to say, if equal measures of each be placed in two evaporating dishes kept side by side, at the same temperature, the ether evaporates in about one-sixth the time of the chloroform; and when the two liquids are mixed, although they then evaporate [369/370] together, the ether is converted into vapour much more rapidly; and, in whatever proportions they are combined, before the whole is evaporated the last portion of the liquid is nearly all chloroform: the consequence is that at the commencement of the inhalation the vapour inspired is chiefly ether, and towards the end nearly all chloroform: the patient experiencing the stronger pungency of ether when it is most objectionable, and inhaling the more powerful vapour at the conclusion, when there is the most need to proceed cautiously.
A death which occurred during a surgical operation in America, has been attributed to the mixture of chloroform and ether which was employed;156 but there is no doubt that the patient died of hæmorrhage. Dr. R. Crockett, of Wytheville, Virginia, removed a fatty tumour from the back of a boy, aged five years. Four parts of washed ether by measure were mixed with one part by measure of chloroform, and a drachm of this mixture was poured on a funnel-shaped sponge which was applied near the mouth and nostrils. The tumour was very large, and required two incisions of nine inches in length for its removal. Six arteries required to be tied; and just as the last one was secured, the child began to vomit. He was found to be pulseless, and he died three or four minutes from the commencement of vomiting. Dr. Kincannon, who was present, and watching the patient, said that up to the time he began to vomit, there was nothing in the circulation or respiration to produce the least apprehension.
The operator said that the patient probably lost four ounces of blood, certainly not six. It must be observed that as the blood during an operation is carried away by the sponges, it is impossible to estimate the amount. It could be ascertained only by an analysis of the water in [370/371] which the sponges are washed. But even admitting that in the present case the loss of blood did not exceed six ounces, it is probable that this amount, flowing suddenly from a child of five years of age, might cause death. Vomiting does not take place when a patient is deeply under the influence of ether or chloroform, and the fact of no signs of over narcotism having appeared, confirms the view that death was occasioned by the loss of blood. [371/372]
This substance was discovered and described in 1844 by M. Balard, Professor of Chemistry to the Faculty of Sciences of Paris.157 M. Auguste Cahours had given this name five years previously to a product which is isomeric with amylene, and is produced at the same time, but is now termed paramylene.
Amylene is made by distilling amylic alcohol with chloride of zinc. The amylic alcohol is obtained from crude fusel oil, otherwise called oil of grain, or oil of potatoe spirit. The fusel oil must be submitted to a careful distillation, with a thermometer in the retort. It begins to boil at a comparatively low temperature, but that portion only is to be retained which comes over from 266° to 284° Fah. Caustic potash is added, to decompose the œnanthic ether which the distilled liquid contains, and it is then redistilled, and that portion which boils steadily at 270° Fah. is collected as pure amylic alcohol. Amylene can be obtained from amylic alcohol in the same manner that olefiant gas, or ethylene, can be made from common alcohol, namely, by heating it with dishydrating agents, as sulphuric, phosphoric, fluoboric and fluosilic acids, and chloride of zinc; but most conveniently with the last substance, which is the one that M. Balard employed. The product which is obtained when amylic alcohol and chloride of zinc are distilled together, contains at least three distinct hydro-carbons, amylene, paramylene, and metamylene; and the amylene [372/373] which is the most volatile is separated from the others by successive distillations.
Amylene is a colourless and very mobile liquid, of extremely low specific gravity; being one of the lightest liquids known. The amylene made for me by Mr. Bullock158 had a specific gravity of 0.659 at 56°. It is very volatile, boiling at 102° Fah. according to M. Balard, and at 95° according to Frankland, and the specific gravity of its vapour is 2.45. It is composed of ten atoms carbon and ten atoms hydrogen, and bears the same relation to amylic alcohol that olefiant gas, or ethylene, bears to common alcohol.
It is inflammable, burning with a brilliant white flame; and in pouring it out by candle light, the same care is required as in dealing with sulphuric ether. A slight explosion may be obtained by applying a light to a mixture of a small amount of its vapour with a large quantity of air.
It is soluble in alcohol and ether in all proportions, but is very sparingly soluble in water, being in fact a hundred times less soluble than many substances which are ordinarily spoken of as insoluble. From a number of careful experiments which I made, I found that water dissolves 2.35 per cent of its volume of the vapour of amylene. It follows therefore, from the specific gravity of amylene and of its vapour stated above, that amylene requires 9319 parts of water for its solution. The water which has dissolved this small quantity of amylene tastes as distinctly of it as amylene itself.
Amylene has more odour than chloroform, but much less than sulphuric ether, and the odour does not remain long in the patient's breath. The smell of amylene somewhat resembles that of wood spirit. The first specimens which Mr. Bullock made were slightly offensive, but the odour improved and diminished in strength, as he obtained the sub-[373/374]stance in a state more nearly approaching to purity. Many persons, who thought the odour disagreeable at first, began to like it after they had been exposed to it three or four times. It is almost without taste, and it produces no irritation, or effect of any kind on the sound skin, even when confined, and prevented from evaporating. The vapour is almost entirely without pungency, furnishing in this respect a remarkable contrast to both ether and chloroform. Its presence can be perceived on first beginning to inhale it, but after two or three inspirations, one cannot tell whether the air one is breathing contains any of the vapour or not. It does not cause any cough unless there is great irritability of the air-passages, or the vapour is breathed of great strength in the very first inspirations.
Amylene produces about as much cold during its evaporation as sulphuric ether does. If a sponge or piece of blotting-paper wetted with amylene is exposed to the air, a portion of the moisture of the air becomes condensed on its surface, by the cold caused during the evaporation of the amylene; and by the further effect of the cold the condensed moisture is frozen, and the sponge or paper is covered with hoar frost.
The boiling point of pure amylene would probably be that which I have quoted above from Frankland, viz., 35° cent. [Celsius] or 95° Fah.; but the amylene which has been obtained for inhalation contains other hydrocarbons of an analogous composition, and its boiling point is not steady: 95° Fah. was indeed about the average boiling point of the greater part of the amylene furnished to me by Mr. Bullock, for it usually commenced to boil at 86°, and as it evaporated, the boiling point gradually rose to 109°, or higher.
No method is at present known of separating amylene from the products which come over with it, except a number of distillations; and although these may be carried so far as [374/375] to obtain a small quantity almost pure, the price of it would be too great to admit of its employment for inhalation. For this purpose, one must be content with a product approaching to purity. Dr. Debout, in an article on amylene,159 says that the boiling point commences at 28° (82° Fah.), and rises gradually to 40° or 45° (104° or 113°) in the best products which have been obtained by Mr. Bullock of London, M. Hepp of Strasbourg, and the house of Ménier at Paris.
M. Duroy published an elaborate paper on amylene, on April 9th, 1857. 160 In this paper, he gives the result of an examination of four specimens of amylene: the first, which he calls A, was amylene made by Mr. Bullock; the second (B) was the amylene of M. Ménier; the third (C) was some that he had prepared according to the process of M. Hepp; the fourth (D) was amylene which he had obtained by a process which he described. In this process, he employed dry chloride of zinc and amylic alcohol. M. Balard recommended a solution of chloride of zinc of a certain strength to be used. I may state, however, that Mr. Bullock had from the first used dry chloride of zinc.
The following table shows the temperature at which the different specimens began to boil, and the temperature to which they rose before being boiled entirely away.

Mr. Bullock's amylene went through the smallest range of temperature whilst boiling away.
M. Duroy found that potassium was oxidized to a certain extent in all these specimens of amylene, and a small quan-[375/376]tity of hydrogen gas was produced, showing that they did not consist entirely of hydrocarbons, but that there distilled over with them a small quantity, either of amylic alcohol, or amylic ether.
The following table shows the cubic centimetres of hydrogen gas which were disengaged from three grammes of each of the different kinds of amylene.
Examined in this way, Mr. Bullock's amylene showed the smallest quantity of impurity; and, next to that, the amylene made by M. Duroy.
M. Duroy found that amylene can be purified from the substances containing oxygen by distilling it again with dry chloride of zinc. He was able to obtain pure amylene, boiling steadily at 35° cent. [Celsius], but to get at this result he made so many distillations that he had only forty grammes of amylene from five litres of amylic alcohol.
He states that the following are the characters of absolute amylene.
To boil steadily at 35° cent [C].
To be without action on potassium, and to preserve that metal like naphtha.
Not to be coloured, even by prolonged contact with caustic potassa.
Not to give rise to valerianic acid under the action of hydrated potassa.
The following table shows the amount of vapour of amylene in air which is saturated with it at various temperatures. The specimen of amylene with which I made the experiments began to boil at 95° Fah. [376/377]

I was not aware of the existence of amylene till 1856, or I should have tried it sooner; for I made inquiry in 1848 for a substance named eupion by Reichenbach, its discoverer, but was unable to obtain it. Eupion is a carbohydrogen, described as having all the physical characters which belong to amylene, though obtained in a different way; and I believe it is the same substance, or the hydride of amyle. Reichenbach obtained it from coal tar, but other chemists have not been able to make it.
Judging from experiments which I had made on analogous substances, there could be no doubt of amylene causing insensibility when inhaled; but I could not tell, without actual trial, whether it might not be unpleasant in its action. [377/378]
I believe that amylene had but rarely been made, and only in very small quantity, until I requested Mr. Bullock to make it for me. For some time afterwards, soon after my first paper had appeared on the subject, M. Berthé, of Paris, made some amylene and submitted it to M. Balard, its discoverer, who acknowleged its purity, and was astonished at the great quantity M. Berthé had obtained. This quantity, however, appears to have only been forty grammes, or about ten fluid drachms.
As soon as Mr. Bullock succeeded in making some amylene for me, I proceeded to perform some experiments with it on small animals. I found that it was necessary that an animal should breathe air containing about 10 per cent of the vapour in order to lose its consciousness, and that 20 per cent caused a deep state of insensibility, whilst 25 per cent could be breathed with perfect safety.
The following are a few of the experiments.
Experiment 43. A guinea pig was placed in a glass jar holding four hundred and twenty-eight cubic inches. Fifteen grains of amylene were dropped through a small tube in the air-tight cover of the jar, fell upon blotting paper suspended within, and quickly evaporated and became mixed with the air. In three or four minutes the guinea pig staggered and became altered in its manner. It did not become further affected, although it was allowed to remain for ten minutes. When taken out its sensibility did not seem impaired. Each grain of amylene produces 1.315 cubic inch of vapour, and consequently the air in this experiment contained 4.6 per cent of vapour.
Experiment 44. The same guinea pig was placed in the same jar three days afterwards, and twenty-five grains of amylene were introduced in the same manner. At the end of two or three minutes the guinea pig seemed estranged in its manner, and turned its head from side to side. In a [378/379] little time it seemed getting drowsy, but at the end of twelve minutes it was still on its legs and moving voluntarily. Eleven grains more of amylene were now introduced. In a little time it sank down unable to stand, and on being turned over by inclining the jar it made efforts to right itself, which became more and more feeble. It was taken out at the end of fifteen minutes, i.e., three minutes after the introduction of the additional amylene. It gave a slight squeak, and moved its feet and eyelids on being lifted. On being pricked it gave decided evidence of sensation. It recovered in a few minutes. There were 7.7 cubic inches of vapour in each one hundred cubic inches of air in the first part of the experiment, and eleven cubic inches in the latter part.
Experiment 45. Six fluid drachms of amylene in a little bottle were put into a glass jar of the capacity of one thousand six hundred cubic inches, and the mouth of the jar was tied over with a large piece of oiled silk. The bottle was emptied by inclining the jar, and the amylene was made to run about the sides of the jar till it had all evaporated. A guinea pig was then folded in the superabundant oiled silk beyond the string which tied it, the string was then opened, and the animal introduced into the jar without allowing any communication with the external air. The guinea pig began to be affected within half a minute, and in a minute it was lying insensible, but moved its limbs when it was rolled about in the jar. In two minutes it was flaccid, and could be rolled about without causing any resistance or muscular action. It lay relaxed and motionless till taken out at the end of four minutes, although by an occasional motion of the eyelids it seemed not altogether insensible. It was quickly taken out, but the moment it was removed it began to kick, and being pricked it flinched. It was not able to stand for two minutes, but after this it [379/380] quickly recovered. Six fluid drachms of amylene weigh 240 grains, and produce 315 cubic inches of vapour; consequently there was nearly 20 per cent of vapour in the air in this experiment.
Experiment 46. A guinea pig, a fortnight old, was placed in the jar holding 428 cubic inches, and eighty-two grains of amylene were introduced on blotting paper. It was six minutes in evaporating. The guinea pig became gradually affected, and, a minute or two before the amylene had all evaporated, it was lying unable to walk. It was allowed to remain till ten minutes had elapsed, that is, four minutes after the amylene was all converted into vapour; but it did not, apparently, become quite insensible. The limbs were never quite relaxed, and when turned over in the jar there was a little motion of the limbs and head. There was also a little quivering motion of the limbs occasionally when not disturbed, and at one time it opened and shut its mouth. On its removal, pricking the soft parts of its toes caused sometimes a slight groan. It recovered slowly and gradually. In ten minutes it was quite conscious, but not as brisk as before the experiment. There was 25 per cent of vapour in the air the guinea pig breathed in this experiment.
Guinea pigs have a great tendency to flinch when pricked whilst they are under the influence of amylene. I did not find this to be the case with other animals.
Experiment 47. A lean, starved cat was placed in a glass jar holding 1,600 cubic inches, and 120 grains of amylene were introduced upon blotting paper. The cat became inebriated whilst the amylene was evaporating; and by the time it had all evaporated--which was four and a half minutes--the cat had sunk down in a state of insensibility. The eyes were turned downwards, so as to expose the white; but its limbs were not relaxed. In a minute or two after-[380/381]wards it made no effort when rolled about in the jar. It was taken out at the end of nine minutes from the commencement of introducing the amylene. It was breathing noisily; its limbs were not relaxed; it was totally insensible to pricking of the ears and paws. It began to recover in about a minute: in two or three minutes it flinched on being pricked; it staggered for two or three minutes longer, and in ten minutes it was pretty well recovered. The amylene would produce 158 cubic inches of vapour, or very nearly ten per cent in this experiment.
Experiment 48. A linnet was placed in a jar holding 428 cubic inches, and forty grains of amylene were introduced on blotting paper. In two minutes it had evaporated. Until it had nearly evaporated, the bird was hardly affected, only evincing a desire to escape. As soon as the amylene had evaporated, the linnet lay unable to move, but evincing consciousness and sensibility by the motion of its eyelids and eyes, and by moving its legs when it was turned over by inclining the jar. It remained in this state for three minutes, when eight grains more of amylene were introduced into the jar. The bird almost immediately closed its eyes; and it opened its bill a little, from which a little liquid flowed. The motion of its legs also ceased, and its breathing was slower. It was taken out half a minute after the last portion of amylene was introduced. It seemed quite insensible when removed, but began to recover in a few seconds. When its foot was pricked, twenty or thirty seconds after its removal, it flinched. In two or three minutes it was quite recovered. There were 12.3 per cent of vapour in the air in the first part of this experiment; and 14.7 per cent in the latter part.
Experiment 49. Another linnet was placed in the same jar, and forty-eight grains of amylene were introduced in the same manner. It took nearly three minutes to evapo-[381/382]rate, hoar frost being produced on the blotting paper. The bird began to stagger when the amylene was about half evaporated; and by the time it was all evaporated, the bird was lying apparently insensible, with its eyes closed, and breathing quickly. It was allowed to remain two and a half minutes, during which it did not alter. It was often rolled about by moving the jar; and during the last minute and a half it made no effort, except once or twice a slight motion of the wings. It was taken out two and a half minutes after the amylene had all evaporated. It was quite passive, and insensible to pricking of the toes, for half a minute or so after its removal, when it began to recover, went through a stage of staggering, and was well in three or four minutes. The amount of vapour in the air, in this experiment, amounted to 14.7 per cent.
Experiment 50. Fifty grains of amylene were diffused in a glass jar holding 330 cubic inches, and a linnet was introduced by momentarily moving the lid a little to one side. It was quickly affected, and in about a quarter of a minute was lying quite insensible. It remained so, breathing quickly and naturally, and made no effort whatever when rolled about in the jar. It was allowed to remain three minutes, and there was a slight fluttering motion of the wings just before its removal. It was quite passive when removed, and insensible to pricking of the soft part of the foot. It began to recover its sensibility in three quarters of a minute. In two minutes it was able to stand, and in six minutes it got on the perch. There was twenty per cent of vapour in the air in this experiment.
As amylene boils nearly at the temperature of the blood, that fluid would be able to absorb about one-fifth as much as it would be able to dissolve, when an atmosphere is breathed containing twenty per cent of the vapour, which produces a complete state of insensibility, or the fourth [382/383] degree of narcotism. When ten per cent is breathed, which has been shown to cause the second degree of narcotism, about one-tenth as much vapour as the blood would dissolve must be absorbed. In treating of chloroform and ether, it was previously shewn that the fourth degree of narcotism was caused by one twenty-eighth part as much of these agents as the blood would absorb; and the second degree by one fifty-sixth part. And these were the proportions absorbed of several other agents which are made from ordinary alcohol, and will afterwards be mentioned.
Although the proportion of amylene absorbed is large in relation to the whole quantity which the blood would dissolve, it is a very small amount on account of the extremely slight solubility of the agent. If we estimate the average amount of serum of the blood in the human adult at 410 fluid ounces, as before, then, as amylene requires 9,319 parts of watery fluids for its solution (as nearly as I could ascertain), the quantity of this agent in the system must be rather less than three grains in the fourth degree of narcotism; rather less than a grain and a half in the second degree; and a very little over two grains in the third degree of narcotism, the condition in which surgical operations are usually performed. Amylene is therefore, when absorbed, about as powerful in its medicinal properties as the alkaloids.
The following fact also proves that but a very small quantity of amylene is absorbed. In breathing this agent backwards and forwards from a small bladder containing 200 cubic inches of air, fourteen minims was the largest quantity I could put into the bladder without being rendered unconscious; but in employing a large bladder holding 670 cubic inches, I could put in forty-five minims, and breathe it backwards and forwards for some time without being rendered unconscious. With fifty minims of amylene I [383/384] immediately forgot where I was; but awoke in a minute or two, seated in the same position, and with the bladder in my hand. Fifty minims of amylene would produce between six and seven per cent of vapour in the bladder; and after the air in the lungs became mixed with that in the bladder, there would be rather more than five per cent of vapour in it.
Viewed in the light of the small quantity which requires to be absorbed into the system to cause insensibility, amylene is a very powerful agent; but when considered in relation to the quantity which is consumed during inhalation in the ordinary way, it is very far from being powerful. This arises from the great tension and the small solubility of the vapour, in consequence of which it is, with the exception of a small fraction, expelled from the lungs again without being absorbed. In this respect it resembles, to a great extent, the nitrogen gas of the atmosphere, with which the lungs are always four-fifths filled, while the blood contains but a few cubic inches. It takes from three to four fluid drachms of amylene to cause insensibility in the adult.
I found, by my experiments on animals, that amylene is, like chloroform and some other agents, capable of causing sudden death by over-narcotism of the heart, and paralysis of that organ; but that it is more difficult to cause this kind of sudden death with amylene than with chloroform.
Experiment 51. One hundred and twenty grains of amylene were made to evaporate in a jar holding 330 cubic inches, and a full grown guinea pig was suddenly introduced, the cover being partly removed for a moment. It was allowed to remain for about a minute, when the breathing became of a gasping character. Being taken out, and the stethoscope applied immediately to the chest, the heart could not be heard to beat; and its action did not return, although the gasping continued for about a minute. There [384/385] was nearly 48 per cent of vapour in the air in this experiment, except that a small quantity might escape as the guinea pig was introduced. I had tried guinea pigs with smaller proportions of vapour in the air, but had not succeeded in arresting the action of the heart.
The lungs were rather congested, and the right cavities of the heart were filled, and somewhat distended with coagulated blood.
Experiment 52. A kitten, six weeks old, was placed in a jar holding 330 cubic inches, after ninety-five grains of amylene had been made to evaporate and diffuse itself. The kitten remained three quarters of a minute in the jar, and was suddenly taken out. It was scarcely insensible on its removal, but soon became so. The stethoscope was applied, and the heart was found to be beating rapidly. The kitten quickly recovered.
One hundred and six grains of amylene were made to evaporate in the same jar, and the kitten was quickly introduced, as before, by moving the cover for a moment. It was allowed to remain for half a minute, and removed with the same symptoms and result as before.
The same quantity of amylene was employed, and the kitten was introduced again, and allowed to remain for fifty seconds. On its first removal the heart was not beating, but the kitten was gasping; and just afterwards the heart was heard to be beating rapidly. The kitten quickly recovered.
One hundred and twenty grains of amylene were allowed to evaporate in the jar, and the kitten was introduced again. It was allowed to remain a minute, and was taken out as the breathing appeared to be on the point of ceasing. The heart was beating when the stethoscope was employed, and the kitten quickly recovered. It seemed impossible to kill it with amylene, except by allowing it to remain and inhale [385/386] the vapour, by those gasping inspirations which took place when the action of the heart was arrested, and which restored the action of this organ, when the kitten was withdrawn from the vapour. In the different parts of this experiment there were 37, 42, and 47 per cent of amylene in the air.
When mice are placed in air containing 30 per cent and upwards of vapour of amylene, they usually recover, as in the following experiment, if the breathing has not entirely ceased on their removal; whilst if they are placed for a quarter of a minute in air containing 8 or 10 per cent of vapour of chloroform, they generally die, although they may be breathing well, and hardly insensible, when they are removed.
Experiment 53. Eighty grains of amylene were introduced into a jar holding 330 cubic inches, and when it had evaporated, a white mouse was introduced. In about five seconds it was quite insensible, and in about a quarter of a minute the breathing appeared to have ceased. The mouse was quickly withdrawn, and immediately began to gasp. After a few gasps the quick breathing returned. In half a minute after its removal the mouse was recovering, and it was soon quite well. There was 32 per cent of vapour of amylene in the air in this experiment.
I administered amylene with the inhaler which I had used for several years in exhibiting chloroform, and which I have described in treating of that agent. In administering chloroform it is desirable that the patient should breathe 4 or 5 per cent of the vapour in the air he inspires; and the air, when saturated with vapour of chloroform at 60°, contains 12 per cent, or nearly three times as much as the patient ever requires. In administering amylene for surgical operations, it is desirable that the patient should take in 15 per cent of the vapour with the air he breathes; and [386/387] air, when saturated with this vapour at 60°, contains 465 [sic; should be 46.5] per cent, or fully three times as much as the patient ever requires. It therefore seemed reasonable that the inhaler which had answered so well with the former agent, might be employed in the same manner, and used successfully with the latter agent. Vapour of chloroform, when inhaled of twice the proper strength, i.e., of 8 or 10 per cent, is capable of causing sudden death by over-narcotism of the heart; but amylene is required to be of nearly 40 per cent, or more than twice the proper strength, before it could produce this result: and it seemed, therefore, reasonable to expect that the inhaler which had been employed for so many years with chloroform, might be employed in exhibiting amylene with an equally satisfactory result. And if the amylene furnished for inhalation had been a constant and uniform product, boiling steadily at the same temperature, like chloroform, there is no doubt that these expectations would have been fulfilled.
I first administered amylene, in King's College Hospital, on the 10th of November 1856, to two boys, about fourteen years old, previous to Mr. Samuel Cartwright extracting some teeth. I had but a few drachms, and being very sparing of its use, it did not entirely remove consciousness in either case, and the pain was not altogether prevented: the effects, however, as far as they extended, were so favourable as to encourage a further trial, which was made in the same institution, on December 4.
On this occasion I exhibited the amylene to four patients--two men, a young woman, and a girl of ten years old: it occasioned complete unconsciousness and absence of pain in each case. The first man was about thirty-five years of age. Half a fluid ounce of amylene was put into the inhaler, and he inhaled for three minutes. At first the valve of the face-piece was about one-third open, but it was gradually moved [387/388] till it was almost closed. The man breathed readily, without coughing, and in a very little time seemed to be unconscious. The pulse became quick and slightly irregular; the skin became flushed; and in about two minutes there was a rather free sweating of the forehead; the eyes did not turn upwards; the conjunctivae did not become insensible; there was no relaxation of the limbs, and, on the contrary, no struggling. The patient sat well, supporting himself, without any tendency to slide out of the chair; the mouth was partly open, and there was a tendency to laugh, just as the amylene was discontinued. The tooth was extracted by Mr. S. Cartwright, without making him flinch or cry in the least. In less than a minute he awoke. He looked a little strange at first, but immediately remembered all the circumstances of his situation, but knew nothing of the operation; and, three minutes after the extraction of the tooth, and six minutes after entering the room, he went away feeling, as he said, quite well. The amylene put into the inhaler was nearly used.
A young man, about twenty years old, next inhaled the same quantity, in exactly the same manner, for just three minutes; there was no irregularity of pulse, and no sweating; otherwise the symptoms were exactly the same. The tooth was extracted without his knowledge, and without causing a cry or flinch. He awoke, and was able to go in three minutes.
A young woman in bad health, an out-patient of one of the physicians of the hospital, next inhaled. She breathed the amylene for four minutes, and about three drachms were used. The effect was carried to the commencement of the third degree of narcotism; and the eyes were inclined to turn up, but did not do so persistently. The edges of the eyelids also remained sensible. There was a little trouble and delay in getting the mouth open, as the muscles of the [388/389] jaws were rather rigid; and when the tooth was extracted, she flinched, and cried out a little. She did not remember the operation. She said she had had a very unpleasant dream, and she was dizzy and uncomfortable for about ten minutes, after which she was better.
A little girl ten years old inhaled for four minutes, and between two and three drachms were used. The eyes were turned up for a short time. She did not flinch or cry as the first tooth came out, but did both as two others were afterwards extracted. She did not, however, know anything afterwards of the operation. She recovered her consciousness in a minute or two, and quite recovered from the effects of the vapour in a few more minutes. There was no sickness, and no increased flow of saliva, in any of the cases.
On December 11th, I administered the amylene again in five more cases of tooth-drawing, with very similar results to those obtained in the previous cases; and on December 13th, I exhibited it in some more important cases.
Mr. Fergusson performed an operation for fungus of the testicle; Mr. Bowman removed some diseased glands from the groin; and there were two cases of tenotomy, in one of which forcible extension of the knee was made.
From November 1856 to July 1857, I exhibited amylene in 238 cases. There were seven cases of lithotomy; six of the patients were children, and the seventh a young man of seventeen. They all recovered. Five of the operations were performed by Mr. Fergusson, in King's College Hospital; and two were performed in St. George's Hospital, by Mr. H. C. Johnson and Mr. George Pollock.
There were five cases of resection of the knee; three of the patients got well, and two died. These operations were performed in King's College Hospital, one of them by Mr. Partridge, and the other four by Mr. Fergusson. Of the seventeen cases of resection of the knee, mentioned at page [389/390] 280, in which chloroform was administered, I know the result only in thirteen of the cases. Of these, eight recovered, one of them after undergoing subsequent amputation at the thigh; and five died.
Some statistics of this operation have been gathered by collecting the cases which happen to be reported in the medical journals, but such statistics are likely to be extremely erroneous. The cases that are reported are probably far more favourable than those that are not reported. A surgeon undertakes an operation of this kind with no other view than the benefit of his patient, and without thinking of the medical journals; and, if his first or second case is unsuccessful, he is probably not inclined to repeat the operation. If the cases should be successful, however, he is inclined to repeat the operation when opportunity occurs, and may ultimately give the result of his experience to the profession.
Mr. Bowman removed the head of the femur in two little boys to whom I administered amylene; they both recovered, as did a girl who inhaled amylene whilst Mr. Fergusson performed resection of the elbow. I administered amylene in four cases of amputation of the thigh: one of these operations was performed by Mr. Henry Lee, on January 7th, 1857, on a girl aged twelve or thirteen, who underwent resection of the knee on the 1st of November previously. That operation was performed by Mr. Bowman, and the girl inhaled chloroform. At the time of the amputation, she was suffering from pyæmia, was extremely weak, and had a pulse of 150 in the minute. The vapour was exhibited to the patient in bed, before her removal to the operating table. There was an examination of the knee before the operation; and the anæsthesia was kept up till the dressings were applied, which was twenty-five minutes from its commencement, and nearly three fluid ounces of [390/391] amylene were used. She went through the operation extremely well. There was no sign of pain, and the pulse remained the same throughout the operation, and there was no depression. The patient recovered.
There was one operation of amputation below the knee by Mr. Fergusson, in which I administered amylene. The patient was a woman of twenty. The operation was performed on account of paralysis of the muscles of the leg and foot. She recovered. There was an amputation of the forearm; two amputations of the great toe, with its metatarsal bone; and two or three of toes and fingers: four cases of operation for stricture of the urethra by perinæal section--three of them by Mr. Fergusson, and one by Mr Curling. There were three operations of lithotrity, two for hæmorrhoids and prolapsus ani, and four for fistula in ano. There were nine operations for the removal of tumours of the female breast; there were seventeen operations for necrosis of the tibia, femur, lower jaw, and other bones.
I administered amylene in several operations on the eye. There were two operations for cataract by extraction, and one by drilling, performed by Mr. Bowman; eight cases of excision of the eye by that surgeon, as well as some operations for artificial pupil, for the removal of foreign bodies from the eye, for staphyloma, and one for the separation of the eyelids from the globe. There were also twelve operations for strabismus, eleven of them by Mr. Bowman, and one by Mr. Fergusson.
I exhibited amylene in forty-eight operations of tenotomy. Several of them were performed by Mr. Fergusson, but the greater number were performed by Mr. W. Adams and the late Mr. Lonsdale, in the Orthopædic Hospital. The narcotism was scarcely carried beyond the second degree in any of these cases. The eyes were open, and the features generally had an expression as if the mind was [391/392] active on some subject or other. The muscles were nearly always in a state of tension, at least they were not relaxed in any case. Many of the patients were children, and a number of them only inhaled between one and two minutes. There were five operations for the forcible extension of stiff joints, and two for dislocation of the humerus: the latter were treated in the St. James's Parochial Infirmary. The first case was a dislocation downwards in a woman aged sixty-eight. She inhaled for three minutes, when, extension being made, the bone slipped into its place with the utmost ease, although Mr. French had found a good deal of resistance in an attempt he made just before sending to me--not any serious resistance or pain, but so much of both as led him to think it would be a good opportunity for trying the amylene. In two minutes after the reduction of the dislocation, and five minutes after beginning to inhale, the patient was quite awake again, and said that she had felt nothing. The other case was a dislocation forwards in a man aged seventy-two. No attempt to reduce it was made till the amylene was administered. The case was under the care of Mr. Buzzard. After inhaling two or three minutes, the old man got into a state of muscular rigidity, and did not get beyond this state, although I continued the inhalation nearly ten minutes, until about two ounces of amylene were used. He was quite insensible, but the rigidity prevented the reduction of the dislocation. So I discontinued it, and sent for some chloroform, which I administered a few minutes afterwards. It produced muscular rigidity rather stronger that that which the amylene had caused; but, by continuing the inhalation steadily for about two minutes, the limbs became relaxed, and the humerus slipped easily into its place. This is the only case in which the amylene has not effected the purpose for which I have exhibited it; and I have no doubt that I [392/393] could have produced relaxation of the voluntary muscles by increasing the strength of the vapour the patient was breathing; for I have always been able to produce relaxation of the muscular system of animals with it; but there were one or two circumstances which at the moment stood in the way of this. The patient's face was so hollow from his loss of teeth that the face-piece fitted badly; and, as it was early in a frosty morning, the water-bath of the inhaler was colder than usual. These defects could have been remedied if necessary, but I thought it as well to use chloroform; and I am inclined to think that chloroform and ether are better agents to employ in those instances where relaxation of the voluntary muscular system is required.
Sixteen tumours of different kinds were removed from different parts of the body, in addition to the tumours of the breast previously mentioned, in cases in which I administered amylene; and there was also a number of miscellaneous operations which I have not mentioned.
One of the patients of the late Mr. Lonsdale at the Orthopædic Hospital was a girl of seventeen, who had the scapula drawn up in an extraordinary manner by the action of the muscles. When she became unconscious from the amylene the shoulder came into its right position, with hardly any pressure, although her muscular system was not in the least relaxed from the action of the vapour; and the deformity remained absent for three days. The amylene was repeated three or four times with the same temporary benefit, and chloroform was given on one occasion when I was not present with a similar result. I have not heard of the subsequent progress of the case. I cannot suppose that the direct effect of amylene would remain three days on the nervous system, and I conclude that the result was brought about by some change in the emotions of the patient.
I gave amylene in twenty-four cases of tooth-drawing, [393/394] including those which were previously mentioned. One of the cases was that of a lady under the care of Dr. Oldham. She was suffering from a large ovarian tumour, and was unable to rise from the sofa. Mr. Bell extracted four teeth whilst she was under the influence of the amylene. She became insensible without the least excitement, was perfectly quiet during the operation, and recovered in a minute or two, feeling quite cheerful and well.
I have administered amylene in seven cases of labour. The first patient was under the care of Mr. Buzzard in St. James's Infirmary, on January 20th, 1857. It was the patient's second labour, and was a lingering one, having lasted thirty-five hours. I administered the amylene only during the last twenty minutes preceding the birth of the child, the head being advanced so as to rest on the perinæum. The vapour was given, well diluted, at the beginning of each pain. The patient breathed very deeply, and got relief very quickly from each pain; the mind was quite clear between the pains, and I could not tell whether or not the consciousness was removed for half a minute or so during each pain. Half a fluid ounce of amylene was used. The next case occurred in an out-patient of King's College Hospital, under the care of Mr. Meadows, Dr. Farre's assistant. It was the patient's third confinement. I arrived three hours after the commencement of labour, and two hours before the birth of the child. The os uteri was almost dilated on my arrival, and the pains were very strong, recurring every three minutes or so. They continued to increase in strength to the last. The patient was probably unconscious for a brief period during the uterine contractions, while the amylene was administered, but between the pains she was quite conscious. Under the use of chloroform, in a labour with brisk and frequently recurring pains, as in this case, the patient usually sleeps on from one [394/395] pain to another. The amount of amylene inhaled in this case was three fluid ounces. The quantity used in each of these cases must have been about half a fluid drachm in each pain, and this is the quantity I had previously recommended Dr. Tyler Smith to employ, when he did me the honour to ask me some questions about amylene before he employed it in a case of labour. The results arrived at by Dr. Tyler Smith, in a case in which he employed amylene, were similar to my own, viz. relief of suffering during the uterine contraction, consciousness between the pains, and no interference with the progress of the labour.
On April 28, 1857, I administered amylene in Brownlow Street, Drury Lane, to a woman in her sixth labour, attended by Mr. Ponsonby R. Adair, one of Dr. Farre's assistants. She had been in labour since three P.M. the previous day. The os uteri was fully dilated, and the amylene was commenced at 5:25 A.M., and continued till 5:50, when the child was born. The placenta was expelled in a few minutes with very little bleeding. The amylene was exhibited with the inhaler at the beginning of each pain, which it soon relieved, although the patient did not become unconscious. The pains came on every two minutes or so, and kept increasing in force till the birth. About six drachms of amylene were used.
On May 1st., I administered amylene to another woman in her sixth labour, also attended by Mr. Adair. The vapour was commenced at 9:30 P.M., the patient having been in labour a few hours. The os uteri was not fully dilated. The pains came on regularly every three minutes, but were not very strong; they, however, gradually increased, and the child was born at half-past eleven. The cord was round the neck, and the child was nearly asphyxiated in the birth, but it was restored readily by Dr. Marshall Hall's method. The placenta was expelled a few minutes after the child [395/396] with very little hæmorrhage. The patient inhaled with every pain, which was very quickly relieved. The last quarter of an hour, she seemed to be altogether unconscious. About three fluid ounces of amylene were used.
On May 14th, I exhibited amylene for about an hour to a woman in her third labour, attended by Mr. Adair. The os uteri was nearly dilated when I arrived, and the patient had been in labour about ten hours. The pains occurred every three or four minutes, but were not strong. Amylene was inhaled with each pain for about an hour, when the pains almost ceased, just as the os uteri was fully dilated. I waited for half an hour without giving amylene, and then left to attend to another engagement. Mr. Adair informed me that the pains returned soon after I left, and that the child was born in about half an hour. The patient was hardly rendered unconscious by the amylene. Between two and three fluid ounces were used.
I exhibited amylene for an hour and ten minutes, on May 25th, to a woman aged 20, in her first labour. She was attended by Mr. Adair. She had been in labour since three P.M. the previous day, and the os uteri was not fully dilated. The amylene was commenced at 9:30 A.M., and inhaled with each pain, which it relieved in a very manifest way. The pains recurred every two minutes and a half. I left off giving the amylene at 10:40 to attend to other business. Mr. Adair informed me that the labour was concluded at one P.M.
On July 1st, I exhibited amylene to a woman in labour with her third or fourth child. Labour commenced at midnight of June 27th, and continued during the following day till the os uteri was dilated to the size of a crown piece, when the pains subsided on the evening of that day, and did not return to be effectual till the evening of July 1st. The amylene was commenced at 10:25, the os uteri being [396/397] almost dilated, and the pains recurring every three or four minutes. The uterine contractions increased in force and frequency, and the child was born at 11:45. There was a gush of blood two or three minutes after the birth of the child, and Mr. Adair introduced his hand and removed the placenta, which was only partially detached. The hæmorrage immediately ceased. The patient was feeble and emaciated, and had suffered repeated beatings by her drunken husband. She recovered favourably, as did the other patients.
The action of the amylene was very favourable in these obstetric cases. The pains were relieved very promptly by it, generally by the time the patient had taken two or three inspirations, and the effect of the vapour passed off in most cases between each pain.
The great ease with which amylene can be breathed, owing to its entire want of pungency, is a decided advantage which it possesses over both ether and chloroform. Insensibility can always be induced with amylene in as short a time as is desirable, namely, in from three to four minutes in the adult, and about two minutes in young children. It is not desirable to cause insensibility in a shorter time than this with any agent. If narcotism is induced too quickly, the symptoms are not uniform or in regular order, owing, no doubt, to the circumstance that the narcotic vapour is not equally distributed through the blood, which must convey it to the nervous centres. Insensibility can, indeed, be generally induced with chloroform in the time above-mentioned, but there are many cases in which there is considerable delay at the commencement of inhalation, owing to the pungency of the vapour, especially in nervous and in sensitive patients, and in persons with irritability of the air-passages from chronic bronchitis, phthisis, or any other cause.
In the use of amylene, absence of pain has been obtained [397/398] with less profound coma than usually accompanies the employment of chloroform and ether. There are some cases, indeed, in which the minor parts of an operation, under these latter agents, may be performed without pain while the patient is in a semi-conscious state, or even altogether conscious, but they form an exception; while in the use of amylene, the patient has very often been half-conscious during the operation. In operations under chloroform, the patients usually indicate the necessity of repeating the inhalation by a tendency to flinch or cry, without showing any signs of consciousness; but in the use of amylene, they have more frequently begun to look about and to speak before showing any sign of pain. There are some patients who will not lie still under the surgeon's knife while chloroform is being used, unless its effects are carried so far that the breathing is on the borders of being stertorous, but I have not met with any such case in using amylene.
The greater number of the operations under amylene were performed while the patient was in the second degree of narcotism, being apparently awake, although not really conscious of surrounding objects. This usual absence of coma in the employment of amylene cannot be looked on otherwise than as an advantage. It must conduce to the safety of the agent when the proportion of vapour in the air is properly regulated. The reason why no accident is known to have happened from chloroform, in the practice of midwifery, when superintended by a medical man, is no doubt due to the circumstance that it is only requisite to induce a slight effect, in comparison with the effect required in surgical operations.
The best indication that the patient will quietly bear an operation under chloroform, is the more or less complete absence of sensibility of the ciliary edge of the eyelid; but during the inhalation of amylene the patient is often entirely [398/399] regardless of the surgeon's knife, whilst the edges of the eyelids retain their full sensibility, and the slightest touch causes strong winking. In operations on the eye, however, and in all other cases where great steadiness on the part of the patient is required, I have thought it best to continue the amylene till the sensibility of the margin of the eyelids was almost abolished; and to effect this it has usually been requisite to carry the influence of the vapour as far as the beginning of the third degree of narcotism, or that condition in which there is no longer voluntary motion of the eyes, or any other part, and in which the eyelids are usually closed, and the pupils inclined upwards. But even in these cases the patient has usually reverted to the second degree of narcotism before the end of the operation, and has shown signs of ideas by the voluntary motion of the eyes and eyelids, or in some cases by speaking. In several cases, however, the sensibility of the eyelid has been removed in the second degree of narcotism; and important operations have been commenced before the patient was "off", to use an expression familiar on these occasions. One instance of this kind was the operation of lithotomy by Mr. Fergusson, on the 14th of March, 1857, in a young man, aged 17, in King's College Hospital. The sound was first introduced, and the stone being detected, the assistants were requested to tie the patient up; and finding his limbs somewhat rigid, they requested me to give him some more vapour. If I had been using chloroform I should have done so without any request, in order to cause relaxation; but I allowed the effect of the amylene to partially subside, and in less than a minute the bandages could be easily applied. I then proceeded to give a little more amylene, but soon found that the margin of the eyelids was insensible; so the operation was performed whilst he was calmly looking about, as if awake; but he showed no sign of pain, and knew nothing [399/400] of the operation. I never saw a capital operation performed on the adult, under the influence of chloroform or ether, whilst the patient was in this condition; but I once administered chloroform in St. George's Hospital to a child of three or four years old, which was cut for stone whilst lying calmly with its eyes open, and holding a toy in its hand, all the time of the operation, without letting it fall.
The pulse is almost always increased in frequency and force during the inhalation of amylene,--especially during the early part of the inhalation, and to a greater extent than happens with chloroform. The respiration is very often accelerated during the inhalation,--about as often, I think, as with ether, and more frequently than with chloroform. In many of the early cases in which I administered amylene, the pupil was dilated for a short time; but I consider that this arose from giving the vapour rather stronger than is desirable. I afterwards gave it more gently, and very seldom observed the pupils to be dilated. They remained, as nearly as I could tell, of the natural size, and also sensible to light, in the cases where I made an observation on that point.
The colour of the countenance is generally heightened more or less during the whole period of the inhalation, and in a few cases there was sweating,--a symptom met with now and then under the influence of chloroform and ether. Amylene does not cause the great increase in the flow of saliva which is so often met with during the inhalation of chloroform, and especially of ether.
There is a tendency to laugh during the inhalation of amylene much more frequently than during the use of chloroform. It occurs just after the patient has lost his consciousness, but is soon subdued by the increasing effect of the vapour. I only met with strong mental excitement in a very few patients, chiefly females. It subsided in half a [400/401] minute in one case, on leaving off the vapour, and did not recur when the inhalation was resumed. In the other cases it was subdued by continuing the inhalation.
The expression of the countenance generally remains calm and cheerful during the action of amylene; but in a few instances there is a singular, and even unpleasant, aspect of the face for a short time, arising apparently from a brief spasmodic action of the muscles.
I met with less rigidity and struggling during the administration of amylene than in the use of chloroform; but this probably arose from the circumstance that the effects of amylene were very frequently not carried to that degree in which rigidity and struggling are liable to appear. It is in the third degree of narcotism from narcotic vapours that rigidity is met with in those cases in which it occurs, but the greater number of the operations under amylene were performed in the second degree of narcotism. The rigidity from amylene, when it occurs, is of a somewhat different kind, and takes place in patients in whom we should not expect it from chloroform. In the spasm and rigidity from the latter agent, the head is more commonly bent forwards or turned to one side, although it is occasionally thrown back; but under amylene, the latter is the usual position it assumes when rigidity occurs, constituting a brief opisthotonos. The rigidity under the influence of chloroform is usually accompanied with struggling, while in that caused by amylene the patient is generally quieter. The persons in whom rigidity and struggling are most violent from the effects of chloroform are lean, muscular men, who work at hard labour, or follow athletic sports, such as hunting, and especially boating; while those who lead a sedentary life, or are reduced by illness, seldom exhibit these phenomena. Women and children seldom exhibit any rigidity under chloroform, and fat persons least of all. Old people do [401/402] sometimes, especially if thin. Under the use of amylene, on the other hand, I have most frequently met with some amount of rigidity in children and young persons, while many robust men, in whom it would be almost certain to occur under chloroform, have not shown any signs of it. The cause of this probably is, that the operation has generally been performed without carrying the narcotism beyond the second degree, while rigidity does not take place till the third degree is attained. In every case where rigidity and struggling have occurred in the employment of chloroform, however violent these symptoms might be, I have continued the vapour gently and steadily till they were subdued, either by removing the tendency to these symptoms, or by carrying the narcotism to the fourth degree, which is accompanied by relaxation of the voluntary muscular system, and usually with some tendency to stertor. In the use of amylene, on the contrary, I have not attempted to subdue the spasm by continuing the inhalation, but have, with the exception of a case of dislocation previously mentioned, withdrawn the vapour when the rigidity appeared, and the operation has either been performed at once, or else, if it was of a nature that the spasm would interfere with, I have waited a short time, and exhibited a little more vapour very gently, so as to get a state of anæsthesia without the recurrence of the spasm.
Mr. Jones, of Jersey, favoured me with the following account of a case in which amylene acted much more favourably on his patient than chloroform.
John D., æt. 41, stout and of very ruddy complexion, so injured his leg that it was deemed advisable to saw off the fractured ends of the tibia. Chloroform was at first given (March 16, 1857), but the effect it produced, though administered with the utmost caution, was evidently of so dangerous a nature, that it is more than probable that death [402/403] would have resulted had it been persevered in longer than five or six minutes (the period it was employed). The patient became quite apoplectic, and had two or three very severe convulsions. Amylene was at once substituted, and with the happiest result. The patient appeared conscious, but was not so, and the operation, which was a tedious one, was commenced and finished without his experiencing the least pain, indeed without his having the slightest knowledge that operative measures had been resorted to.
Amylene differs widely from chloroform, and still more from sulphuric ether, in the promptitude with which patients generally recover from its effects. This is a character of amylene which might have been predicted from its physical properties. I have many times observed how quickly, and, indeed, almost instantaneously, small animals recover from the stupor occasioned by certain permanent gases which are sparingly soluble in watery fluids, as olefiant gas, carbonic oxide and carbonic acid gases, nitrous oxide and the gaseous oxide of methyle. Now amylene is so volatile as to approach to a permanent gas; at a temperature a little above that of the human body it would be a gas, and the vapour is very sparingly soluble in watery fluids, and consequently in the blood. Sulphuric ether is, indeed, as volatile as amylene. I cannot remember any other two bodies whose volatility is so nearly alike but sulphuric ether is very soluble in watery fluids, in comparison with amylene. Water dissolves a tenth of its volume of liquid ether, or 23 volumes of the vapour. Consequently a large quantity of ether is absorbed during inhalation, and the blood has to pass many times through the lungs before it is freed from it. The quantity of amylene which is absorbed is, on the contrary, extremely small, as I have explained above, and this, together with its volatility, is no doubt the reason why the patient recovers so promptly from its influence. In about a minute after [403/404] the operation is concluded, and the inhalation left off, the patient usually awakes from the influence of amylene, and completely recovers his consciousness. The same quick recovery may take place after chloroform, but more frequently it is a few minutes before the patient is quite conscious. I have seen two or three instances in which a child has slept for twenty minutes or half an hour after amylene, but it must be remembered that children sometimes sleep for hours after chloroform in cases where the operation has not produced a painful wound. The quick recovery of the patient is a decided advantage in all minor operations. In great operations, where the patient is obliged to keep his bed afterwards, it is of less consequence whether he wakes promptly or not, although, even under these circumstances, his friends are generally anxious to see him recover his consciousness. The smarting of the wound after an operation is often prevented longer when chloroform has been employed than after the use of amylene, and this may be considered as a slight advantage which chloroform possesses in certain cases. In some instances, however, in which chloroform has been used, the patient begins to show symptoms of suffering pain in the wound before he has entirely recovered his consciousness, while after amylene I have not seen symptoms of pain in the wound till consciousness had completely returned. In any cases where the pain after an operation, either from a wound or ligatures or caustic, is very great, the inhalation of the agent which has been employed may be gently repeated at times until the pain has a tendency to subside, or till an opiate shall take effect.
The patient generally seems surprised or confused on first recovering from the effects of the amylene, but in a few seconds he becomes, in most cases, completely conscious of his position, and feels that his mind has been wandering. He often says he does not know where he has been in his [404/405] dreams, or that he has been a long way. Sometimes he does not remember exactly what he has dreamed about; at other times he does. All this is common enough after chloroform, except that the process of recovery is generally much slower; but there is one condition of mind which is very common after chloroform, which I have rarely met after amylene, I allude to that condition in which the patient asserts that the vapour has not taken effect, and that he has not been asleep at all.
Amylene appears to support the pulse under loss of blood at least as well as chloroform. I have not found the pulse to fail, although there was rather free hæmorrhage in some of the operations.
There has been a little headache in a few of the cases as the effects of this agent were subsiding, but it passed off in a few minutes.
In administering amylene, the vapour must be given of such a strength as will cause insensibility in about three minutes, or it will not succeed at all unless the strength of the vapour be altered. In giving chloroform, the vapour may be of less than half the desirable strength, and by continuing more than twice the usual time, the patient may be rendered insensible; and in using sulphuric ether, the vapour may be breathed of one-seventh the proper strength, and by continuing it constantly for seven times the usual period, i.e., for half an hour, the patient might be rendered insensible; but in using amylene, time will not make up for deficiency in the strength of the vapour. If the vapour be not strong enough to cause insensibility in about three minutes, it might be breathed for an indefinite period without causing insensibility; and the patient is solely affected by what he has inhaled within two or three minutes.
On account of the very rapid subsidence of the effects of amylene, it requires to be very frequently repeated during [405/406] the performance of an operation. The patient generally requires to inhale a little of it every half-minute or so to keep up its effect. On this account, it is not well adapted for certain operations on the face. I did, however, administer it with complete success in several operations on the face in King's College Hospital. Amongst these, there were four operations by Mr. Fergusson for making a new nose in which I administered amylene, and succeeded in preventing the pain by holding a hollow sponge, wetted with that agent frequently, near the mouth and nose.
In cases of tooth-drawing, in which a number of teeth or stumps have to be taken out, the effects of the amylene are apt to pass off before the operation is completed, and the inhalation has to be repeated once or twice, but in cases when only one or two teeth require to be extracted, amylene has a great advantage in the promptitude with which the patient recovers from its effects. There is occasionally some difficulty in opening the mouth with amylene, as with chloroform.
The patient has nearly always a very cheerful expression of countenance when he recovers from the amylene, and the state of his mind, as indicated by his conversation, corresponds to his look. Dr. Debout has noticed the same circumstances. Speaking of the patients operated on under amylene in Paris, he says, "A leur réveil et le premier moment de stupeur passé, leur physionomie est épanouie." The same state of countenance and mind is met with after chloroform only now and then, and is by no means the rule.
Hysterical symptoms occurred in a few women after operations under amylene. They were met with about as frequently, I think, as after chloroform. These symptoms generally subsided in a few minutes; but in one or two young women in the hospital, they lasted nearly an hour.
The greatest advantage that amylene possesses over ether [406/407] and chloroform, is the great infrequency with which it excites sickness. I only saw vomiting occur in two of the 238 cases in which I administered amylene, although it occurred before I left the patients' room in twenty-two cases out of 100 in which I administered chloroform and kept an account of this symptom, at the time I was using amylene. In the greater number of the cases in which chloroform was exhibited, the patients had been requested not to take a meal; whilst in the cases in which amylene was administered, no directions regarding diet had as a general rule been given.
I made subsequent inquiries respecting most of the patients who inhaled amylene, and I was only able to hear of sickness in eight or ten cases, and it was not distressing or troublesome in any of these. It generally occurred three or four hours after the amylene, and subsequently to the patient taking his first meal after the inhalation. In one of the two cases in which vomiting occurred after amylene before I left the room, there was retching for four hours; but I did not hear of so much sickness after any other case in which I administered this agent; and there was no faintness or depression either in this case or any other in which amylene was employed, although faintness and depression often accompany the sickness which is occasioned by chloroform. Some of the patients who inhaled amylene without being sick, had previously suffered from sickness after inhaling chloroform. I administered amylene, on January 30th, 1857, to a lady, about twenty-five, whilst Mr. Bowman operated for strabismus, and there was no vomiting or sickness, either at the time of the operation or afterwards; but the same patient had undergone a similar operation a week previously, when chloroform was administered, and on that occasion vomiting commenced before the operation was finished, and recurred every quarter of an hour, with violent retching, for twelve hours. [407/408]
I had the misfortune to lose two patients from the inhalation of amylene. The following are the particulars of these cases.
Mr. Fergusson requested me to assist him on the 7th of April, 1857, in the case of a gentleman on whom he was about to operate for fistula in ano. The patient was thirty-three years of age, and was in good health, with the exception of the local complaint, although he had lived somewhat freely. Mr. Fergusson examined the patient's chest the day before the operation, and found the sounds of the heart to be normal. I felt his pulse just before he began to inhale. It was natural, but somewhat accelerated, as usually happens just before an operation. He was lying on his side in bed. About six fluid drachms of amylene were put into the inhaler (I never intentionally used all I put in, but added more before the paper became dry), and he breathed steadily and gently. The valve was gradually advanced over the opening in the face-piece till it about three-quarters covered it, and the patient appeared to become quietly unconscious in about two minutes. He breathed quickly for a few inspirations just as he appeared to become unconscious. Just after this, Mr. Fergusson came and felt the patient's pulse, and he says it was very good. I felt it also. I looked at my watch at this time, and it was two minutes and a half or two and three-quarters from the beginning of the inhalation. Mr. Fergusson commenced to use the probe, and, finding the patient did not flinch, he began to use the bistoury. Mr. P. C. Price assisted at the operation. I held the patient's thigh with one hand, as I often do in such an operation, lest he should flinch. He did not flinch, however, but kept his limbs tense, without moving them. Just at this moment, I observed that the valve of the face-piece, which I had left three-quarters covering the opening, had moved so as to cover it entirely, but I cannot say whether [408/409] or not the patient had taken an inspiration a little stronger than I intended, and thought nothing of the matter, as I have frequently had to close the valve completely in giving amylene. It could not, however, have been many seconds in that position, for I paid no attention to the operation, except so much as was requisite to guide me in what I was doing. The inhalation was discontinued at the moment I have mentioned, and on looking round directly after, I found that the operation, which had apparently been but one incision, was finished. I now began to feel for the pulse, more out of constant habit, and from a scientific curiosity, than from any supposed necessity of doing so. Although it had been good only half a minute before, I could not find it in the left wrist, and only a slight flutter in the right one. His breathing was, however, good, indeed quite natural, and he did not seem even to be very insensible, for there was some motion both of his features and limbs, as if he were about to awake. I watched the patient with great anxiety, thinking that surely his good and natural breathing would restore the pulse, and feeling that at all events this superseded any other measures at the moment. In two or three minutes, however, he seemed to be getting more insensible; he did not wink on the edge of the eyelids being touched, and the breathing was getting slower and deeper. I called Mr. Fergusson's attention to the patient, and both he, who was preparing to go away, and Mr. Price, who had all the time been standing by the patient, were surprised to find that anything could be wrong, as they had seen the patient going on apparently so well, not only during the inhalation, but after it was discontinued. They dashed cold water in his face, which did not seem to have any effect. His countenance was now livid, and his breathing of a gasping character. It soon began to leave off, with the exception of deep, distant, [409/410] gasping inspirations, and we therefore began to perform artificial respiration, by Dr. Marshall Hall's method, placing him in the prone position, and bringing him partly round, while Mr. Price kept the mouth open. The air could be distinctly heard passing through the larynx during this motion. We also tried pressing on the chest with the head on one side and the mouth open, which answered very well as regarded the ingress and egress of air. Inflation from mouth to mouth was tried, but did not seem to answer so well. Although deep gasping inspirations were made by the patient till fully ten minutes had elapsed from the failure of the pulse, the measures used had no effect; I believe that I heard a feeble motion of the heart even after this period; and, as Mr. Fergusson perceived a slight pulsation at the same time in the right wrist, I was probably not mistaken. There were no further signs of life after this, although the artificial respiration was continued for a long time: I am quite sure as to the length of time respiration continued after the failure of the heart's action. The pulse ceased to be distinctly perceptible at ten minutes before five, and the patient was still breathing at five o'clock. He had not taken food for some hours, but drank a pint bottle of ale a little while before the operation. A good portion of amylene remained in the inhaler after it had been uncovered for an hour and a half.
There was an examination of the body forty-eight hours after death. The body was rigid. There was a good amount of fat beneath the integuments. The cartilages of the ribs were ossified. The lungs were large, and did not collapse; they completely filled the cavity of the chest, and seemed by their texture to be emphysematous, although there were no large cells on the surface. There was a little congestion at the posterior surface of the left one, otherwise they were not very vascular. There was a little clear fluid in the pericar-[410/411]dium. There was a good deal of fat on the surface of the heart, which was somewhat larger than natural. It was removed by cutting the great vessels before it was opened, and in removing it three or four ounces of dark-coloured fluid blood escaped. The right ventricle was somewhat dilated, otherwise the heart was healthy; the walls of the left ventricle seemed very thick, but it was contracted, so as almost to obliterate the cavity. The liver was vascular, dark-coloured, and friable. The stomach was healthy, and contained only a little mucus. The other organs were not examined. There was no odour of amylene in the body.
I believe the patient had emphysema of the lungs. There was no such force used in the artificial respiration as could permanently dilate the air-cells, and the dilatation of the right ventricle indicates some chronic obstruction to the pulmonary circulation.
The other death from amylene occurred in St. George's Hospital on July 30th, 1857, in a case in which Mr. Cæsar Hawkins removed a small epithelial tumour from the back. The patient, a short, muscular man, was a tailor, twenty-four years of age, who had been in the Hospital several months, and had had three similar tumours removed, by as many operations, under chloroform; the last of these operations having been performed three weeks previously. He inhaled the amylene without any difficulty; in about two minutes he appeared to be unconscious, and, in another minute, the sensibility of the margin of the eyelids was somewhat diminished, and I told Mr. Hawkins that he might perform the operation. For this purpose the patient, who had been lying on his side on the table, was turned a little more on his face, or at least it was attempted to turn him, when he burst out into a kind of hysterical excitement, laughed loudly, and was with difficulty held on the table. Nothing was done during this excitement, which lasted [411/412] about a minute. After it had subsided, I administered a little more amylene, although the patient had not recovered his consciousness; and then Mr. Hawkins performed the operation, which I believe did not last more than two minutes altogether. During the operation, the patient was turned on his face. He rested, I think, chiefly on his knees and elbows. He was muttering in an incoherent manner, and making slight attempts to move, but was easily restrained. I gave him an inspiration or two of amylene now and then during the operation, with the intention of preventing his waking prematurely; for this purpose, I turned the head a little to one side, and raised the face a little from the table.161 I had concluded that the patient would not require any more amylene, and was expecting that he would show signs of returning consciousness or sensibility almost as soon as Mr. Hawkins had tied the suture which he was introducing; but, instead of this, the limbs became relaxed, and the breathing, though free enough, took on a noisy, snoring character.
This is a state which is common enough in the use of chloroform, and excites no alarm whatever, but I felt that it ought not to occur in the use of amylene, especially after it was left off. I therefore sought again for the pulse at the wrist, and could perceive it only with difficulty, if at all. I spoke to Mr. Hawkins, and we immediately turned the patient on his back. His face had already become livid, and his breathing was of a gasping character. Mouth to mouth insufflation of the lungs was performed, and between the insufflations there were spontaneous acts of inspiration, during which the air seemed to enter the lungs freely. In a minute or two, the lips became of a proper colour, and the countenance had altogether such a natural aspect that the patient seemed to be recovering. The pulse at the [412/413] wrist, however, could not be felt. No one listened to the chest at this time, for fear of interrupting the process of artificial respiration. After two or three minutes, Dr. Marshall Hall's method of artificial breathing was substituted for the insufflation, and it was continued very perfectly by the house surgeons and others for an hour and a half, with the exception of two short intermissions, which will be mentioned. During three quarters of an hour of this time, there were spontaneous inspirations, during which air entered the lungs, in addition to that which entered during the turning process. Twenty minutes after the accident, the process of artificial respiration was suspended for about a quarter of a minute, to enable me to listen to the chest. I thought I could hear the heart beating regularly, but very feebly, and certainly there was a good vesicular murmur, and the air seemed to enter the lungs by the patient's own breathing, almost as freely as in health. At the end of three quarters of an hour, with the permission of Mr. Hawkins, I introduced two hare-lip pins which had been connected with the electro-magnetic battery, with the intention of performing galvano-puncture of the heart. The needles were introduced to the depth of about an inch and a half between the cartilages of the ribs, just to the left of the sternum, and on a level with the nipple. They were afterwards found to have penetrated the walls of the left ventricle, near the septum, but without reaching the cavity. There was a quivering contraction of the pectoral muscle when the needles were first applied, but no effect on the heart. The needles ought probably to have been coated with some non-conducting substance almost as far as their points. There were no further efforts of inspiration after this time, but this was probably only a coincidence. The electro-magnetic battery had been applied in the early part of the treatment by means of the wet sponges applied to each side of the chest, but it produced no effect. [413/414]
An examination of the body was made by Mr. Holmes, the Curator of the Hospital Museum, on the following day. A good deal of dark-coloured fluid blood flowed from the right cavities of the heart, and the left cavities contained but little blood. The heart was pale and somewhat friable; but a microscopic examination by Mr. Holmes did not show any fatty degeneration. The lungs were moderately vascular, and contained some small epithelial tumours of the same character as those removed from the back. There was a large cyst in one kidney; but, with these exceptions, the organs were healthy. The vessels of the brain were not distended, and that organ was altogether less vascular than is usual after sudden death. No smell of amylene was perceived in the body.
The continuance of the respiration so long after the heart was paralyzed in these two cases, and especially in the second one, is a remarkably curious event. The respiration continued after the heart had ceased to act in several cases of death from chloroform, but not for so long a time as in these deaths from amylene. It is probable that there must have been some little circulation going on through the brain whilst the respiration lasted, and in fact, the slight fluttering pulse and feeble sounds of the heart, once or twice perceived, indicate that the circulation was not absolutely arrested. Under these circumstances, we may inquire why the action of the heart does not recover. If the circulation were going on in the coronary arteries, it might be expected that the blood from the lungs, which has been aerated by respiration, and freed from the narcotic vapour, would restore the action of the heart. But it is probable, for the reasons stated at page 262, when treating of accidents by chloroform, that the circulation through the coronary arteries is arrested.
The accident clearly commenced at the heart in both these [414/415] cases, and I believe that the brain was never more than partially under the influence of the amylene in either of them. In the Medical Times and Gazette of July 25th, 1857, M. Devergie is related to have expressed an opinion in the Academy of Medicine of Paris, that the first of the above deaths from amylene was caused, in great part, under the influence of true asphyxia, using that term in its modern acceptation. Now that is altogether an error, arising, probably, from M. Devergie not having seen any original account of the case. There was no cause of asphyxia, either internal or external; the patient breathed well until after his heart had ceased to beat, unless in the most feeble and doubtful manner. The valve which was closed only altered the direction, but not the amount of air. In fact, the patient was throughout supplied with as much air as could enter through a tube twice the size of his windpipe.
I had scarcely any hope of the patient in St. George's Hospital from the very commencement of the accident; for I felt that if he could be recovered by artificial respiration, his own breathing would have remedied the accident, even before it was discovered. From what has been published respecting the pulse sometimes stopping and commencing again, during the inhalation of chloroform, it is probable that many accidents, in which the heart has been nearly paralysed, have happened, and rectified themselves, without attracting much notice.
I have no doubt that in each of these accidents the patient must have taken into his lungs at one moment air containing upwards of thirty per cent of vapour of amylene. And there is no doubt that the cause of this was the unsteady boiling point of the agent. If the amylene with which I was supplied had boiled steadily at the same temperature, there is no doubt that the means which I was employing, and which had enabled me for ten years, whilst exhibiting [415/416] chloroform, to give four per cent of the vapour, probably without ever allowing the quantity to exceed six per cent, would have enabled me to give fifteen per cent of vapour of amylene without permitting the quantity to exceed twenty per cent.
The alteration in the boiling point of a specimen of amylene from 86° to 115° Fah. would cause it to give off more than twice as much vapour in the beginning of its evaporation as towards the end; and, moreover, the different specimens of it did not always possess the same amount of volatility.
The temperature of the external air as it influenced that of the water-bath of the inhaler would have some influence over the evaporation of the amylene, but I altered the amount of evaporating surface of paper according to the season of the year for amylene, as I was in the habit of doing for chloroform. The highest temperature of April 7, the day on which the first accident happened, was at Greenwich, according to the Report of the Astronomer Royal, 62°; and on July 30, the day on which the second accident happened, was 78.7°. After the first accident, I had reduced the surface of bibulous paper in the inhaler to one half of what it had previously been.
The first of the above accidents happened in the 144th case in which I administered amylene, and the second in the 238th case. In the ninety cases and upwards in which I administered amylene between these two accidents, I never had occasion to feel a moment's uneasiness about it.
In the future cases in which I employ amylene, it is my intention to administer it from a bag or balloon, putting in so much of the liquid as will make fifteen per cent of vapour when the bag is filled up with air. In this manner, the variability in the boiling point of the amylene can have no influence whatever on the amount of vapour which the [416/417] patient breathes; and if the vapour be breathed over again, within certain limits, in the manner of nitrous oxide gas, there will be a great saving in the amount of amylene consumed.
In my first paper on amylene, which was read on January 10th, 1857, I said: "While I cannot venture to predict for it the absolute safety which seems to attend sulphuric ether under all circumstances, I trust that it will be perfectly safe with careful management."162 And I added further on, "It is my opinion that the cold produced during its evaporation would, in all the ordinary methods of inhalation, prevent the air from taking up a quantity of the vapour which would be dangerous."
Although amylene was largely used in Paris, Strasbourg, Montpelier, and Lyons, soon after I published my first account of it, and although I have lately heard that it is still employed in Paris and Berlin, nearly eighteen months after its first use in these places, I am happy that I have not heard of any accident from its use except the two which happened in my own hands.
M. Giraldis, of Paris, who was present at the operating theatre of St. George's Hospital when the accident happened at that institution, had already employed amylene in 100 cases in children, and I believe that he continues to use it. Given on a handkerchief or sponge, I believe that amylene is safer than chloroform, owing to the greater cold produced during its evaporation, and the limit thereby put to the amount of vapour which is given off; but I have seldom given it in this manner, as I do not think it would be certain and regular in its action, and any doubt on these points would, with me, have quite overbalanced its other advantages. In applying amylene on a sponge, M. Rigaud of Strasbourg used 100 grammes (between four and five [417/418] fluid ounces) in making an adult patient insensible, although half a fluid ounce suffices with the inhaler I employed.
Mr. Clarke, of Bristol, in a paper which he published on amylene,163 says: "It seemed impossible to get too much into the system, and with this I have been greatly impressed; it is this fact that appears to me to promise an immunity from danger. . . . It requires to be given almost unintermittingly, and requires the same amount of attention to keep up its effects as chloroform does to keep the patient safe. The direction of the attention, however, is one less calculated to give anxiety."
Dr. Debout stated, as the result of some experiments on animals, in which he was assisted by M. Duroy, that if it sufficed to double the quantity of chloroform in order to transform the anæsthetic dose of that agent into a poisonous dose, it was necessary to quadruple that of ether, and to quintuple that of amylene, in order to arrive at the same result; and that, therefore, the innocuousness of the new agent was still greater than that of sulphuric ether.164
In a paper which Professor Tourdes, of Strasbourg, read before the Academy of Medicine of Paris, he came also to the conclusion, from a series of experiments and observations, that "amylene was evidently much less dangerous than chloroform, perhaps even than ether. "165
According to my experiments, amylene ought to be placed between chloroform and ether in respect to its comparative safety by the ordinary methods of administration; and by breathing it from a bag, in the manner previously mentioned, it would be absolutely safe, so long as the right quantity were put into the bag.
Papers on amylene were read to the Academy of Medi-[418/419]cine of Paris by Dr. Debout and M. Tourdes, and were reported on favourably. M. Giraldis afterwards presented a paper in which he stated the very favourable result of seventy-nine cases in which he had employed it. The Academy on this occasion recommended the disuse of amylene on account of the accidents which had happened in my hands, apparently overlooking the circumstance that M. Giraldis himself had been much more successful in the use of amylene than in that of chloroform. M. Jobert de Lamballe, the reporter of the Commission, stated that amylene deprived the blood of its red colour and that chloroform does not. But there is no difference between these agents in this respect; the blood retains its proper colour under the use of either of them, unless the effects are carried so far as to interfere with the breathing. [419/420]
This substance was discovered some few years ago by M. M. G. Regnault. It is made by exposing to the sun's rays a mixture of the vapour of chloride of ethyle (muriatic ether) and chlorine gas. One equivalent of the hydrogen of the chloride of ethyle is replaced by an equivalent of chlorine. Its composition is four atoms carbon, four atoms hydrogen, and two atoms chlorine. It has the same composition as Dutch Liquid, which is made by the combination of olefiant gas and chlorine gas; the specific gravity of its vapour, 3.42, is also the same as that of Dutch liquid, which it resembles also in taste and smell. The boiling point is however different, and it differs from Dutch liquid in not being decomposed by an alcoholic solution of potassa.
I tried several times to make the monochlorurretted chloride of ethyle in 1849 and 1850, but did not succeed in procuring more than a drachm or two at once, owing to the constant over-action of the chlorine and the production of other chlorurretted products. In 1851, however, these products which result from the decomposition of muriatic ether by chlorine gas were recommended in Paris as local applications in rheumatism and other painful affections, and Mr. Mason was kind enough to obtain for me from that capital a pint bottle of a liquid consisting chiefly of the monochlorurretted chloride of ethyle. It was mixed with a certain portion of the bichlorurretted and terchlo-[420/421]rurretted products, but I was able to separate by distillation as much of the monochlorurretted product as enabled me to administer it to twenty-two patients. Mr. Mason was, however, not able to obtain any more liquid containing any of the monochlorurretted chloride. What he afterwards was able to obtain had a very high boiling point, and consisted chiefly of chloride of carbon; carbon four atoms, chlorine five atoms.
The monochlorurretted chloride of ethyle resembles chloroform very much in taste and smell, and in its physiological properties. Its boiling point is 149°, whilst that of chloroform is 140°; the specific gravity of its vapour is also lower; for these reasons, it is considerably less volatile than chloroform, and it is therefore pretty certain that it would not be liable to cause the sudden deaths which have occasionally been produced by the administration of chloroform, even if it were given freely and with no great care. The difficulty of procuring it in a state of purity is, however, a barrier to its introduction into practice.
I first administered this preparation in King's College Hospital, on June 20th, 1851, to a young woman, whilst Mr. Wm. Hewett, the house surgeon, repeated the operation of paring off venereal warts and applying nitric acid. The patient breathed it very readily without appearing to suffer from the pungency. She was a little longer in becoming unconscious than on former occasions from the chloroform, but soon after becoming unconscious, the sensibility of the conjunctiva diminished, and the operation was commenced. There was some flinching, so that she required to be held, but there were no cries or other signs of sensation. Consciousness returned almost immediately, and she seemed more exhilarated than after chloroform. She had had her dinner just before the operation, and at one time, soon after recovering her consciousness, she said that she felt rather [421/422] sick, but this feeling passed off without vomiting, and she did not remember it afterwards. She did not begin to cry out from the smarting till twenty minutes after the operation, when she had been quite conscious, collected, and rational for a quarter of an hour, although on the two former occasions, after chloroform had been inhaled, she began to cry immediately after the operation, and almost before consciousness had returned. Next day she was very well.
On the following day I administered the same preparation to three patients on whom Mr. Fergusson operated in King's College Hospital. The first was a boy seven years old, who had the forefinger removed, together with part of the metacarpal bone, on account of a large enchondroma. The second was an infant three months old, which was operated on for hare-lip; and the third was a woman about thirty-five, who had some venereal warts removed from the pudenda. There was no sickness in either of the cases, although the little boy and the woman had taken their dinners just before the operation.
On June 25th, I administered the preparation with the chloroform inhaler, as in all the other cases, to a muscular young man, about 25, whilst Mr. Henry Lee removed some piles, and applied nitric acid to the raw surface. The patient was six feet three inches in height, and weighed fourteen stone. He became insensible rather slowly, with low muttering and a good deal of rigidity. The operation lasted about ten minutes, during which the inhalation was repeated two or three times. There was no pain. He recovered his consciousness in two or three minutes after the conclusion of the operation; he said that he felt drunk, and he appeared so for a few minutes. He was very cheerful, and had no sickness, although he had had his dinner just before coming to the hospital to have the operation performed. Half a fluid ounce of the monochlorurretted com-[422/423]pound was inhaled, being about the same quantity as would have been consumed of chloroform.
The other operations in which I administered this preparation, consisted of the removal of a tumour situated below the angle of the jaw in a young woman, by Mr. Fergusson; an operation on the tibia and fibula of a little boy, for un-united fracture, by Mr. Bowman; trephining the tibia of a young man, and giving exit to a collection of pus, by Mr. Henry Lee; an operation for necrosis of the tibia, by the late Mr. Avery; two operations for hare-lip; two operations for fistula in ano; one for nævus on the forehead; one for tenotomy; and one for removal of a fatty tumour, by Mr. Fergusson.*
*In the act of writing this last sentence, Dr. Snow was seized with his fatal illness. The sentence required, however, but the addition of a word or two, to render it complete.--(EDITOR [BWR].)
1See Monthly Journal of Med. Sc., vol. viii, p. 452.
3a Natural. Hist., lib. xxv, cap. 13.
3b De Herbarum Virtutibus, cap. 131.
5 De Causis Morb. Diut., lib. i, cap. 6.
5a De Morris Acutis, lib. i, cap. 4.
6 Vet. Acad. Handl., 1763, vol. xxiv, p. 229.
7 Comptes Rendus de l'Acad. de Sc., t. xxviii, 1849, p. 195.
8See Herodotus, book iv, 73-5.
10Med. Gaz., vol. xli, p. 515.
11Observations sur la Physique, tome xvi (1780), p. 256.
12Method of preventing or diminishing Pain in several Operations of Surgery. Lond. 1784.
13 Gazette des Hôpitaux, 1st April, 1854.
14 Hypnotism is the term employed by Mr. Braid of Manchester for the peculiar sleep produced by the Mesmerists.
15 Record of Cases treated in the Mesmeric Hospital. Calcutta, 1848.
16Cary's Herodotus, book i, 202.
19Translated into Latin by Father Angelus, Paris, 1681, p. 21.
21See Medicinal Use of Different Kinds of Airs, by Dr. Pearson. Birmingham, 1795.
22Researches concerning Nitrous Oxide, p. 556.
23See 32nd Congress, 2nd Session (Senate) Rep. Com. No. 421, p. 17.
23b A Defence of Dr. Charles T. Jackson's Claims to the Discovery of Etherization. Boston, 1848.
24The Inhalation of the Vapour of Ether in Surgical Operations. By John Snow, M.D. 1847.
25Pharmaceutical Journal, Feb. 1847, p. 357; and Med. Gaz., 1847, vol. xl, p. 939.
26Quoted in Med. Gaz., 1847, vol. xl, p. 1153.
27Lancet, Nov. 27, 1847, p. 575 ; and Med. Gaz., 1847, vol. xl, p. 1031.
28Dr. Pereira in Pharmaceutical Journal, March 1846, vol. v, No. 9.
28aSilliman's American Journal of Science and Art, vol. xxi, p. 64, Jan. 1832.
29Ann. de Chim. et de Physique, t. xlviii, p. 131.
32Formic acid is so named because it was originally obtained from the red ant (Formica rufa). It is now made from starch.
33Turner's Chemistry, 8th ed., p. 1009.
34Nearly all the chloroform used in Great Britain and her colonies is made in Edinburgh, where the spirit duty is lower than in England. The London druggists have almost ceased to make it, as they find it cheaper to get it from the trade in Edinburgh.
35The Edinburgh druggists suffered a great loss in 1850 from purifying their chloroform in this way on the recommendation of Dr. Gregory, who was not aware of the consequences, although they had been stated by Dumas (Ann. de Chim. et de Physique, t. lvi, p. 117).
36I have seen some specimens of chloroform that left a white, limy-looking stain on the hand, which I believe was a minute quantity of crystalline chloride of carbon. These specimens were unobjectionable for all practical purposes, and had the merit of keeping remarkably well.
37See Med. Gaz., vol. xl, p. 1092.
38Dr. Letheby in Med. Gaz., vol. xlvi, p. 1037.
40Since the above was written, I have met with an instance in which the pulse was only 40 in the minute, as the effects of the chloroform were subsiding. There was neither sickness nor loss of blood. The case was that of a gentleman in good general health, who inhaled chloroform whilst Mr. Brodhurst endeavoured to make forcible flexion of the femur on the pelvis. He woke without any unpleasant symptoms, and the pulse resumed its natural frequency.
41Gazette des Hôpitaux, 20 Mars, 1847.
42Medical Gazette, vol. xli-ii.
43According to Professor Miller, chloroform was given, at one time, in the Royal Infirmary of Edinburgh, in a somewhat slovenly, and not very cleanly manner; he describes the means of applying it as, "anything that will admit of chloroform in vapour being brought fully in contact with the mouth and nostrils; a handkerchief, a towel, a piece of lint, a worsted glove, a nightcap, a sponge." He says, "In the winter season, the glove of a clerk, dresser, or onlooker, has been not unfrequently pressed into the service. The object is to produce insensibility as completely and as soon as we can; and there is no saying, à priori, whether this is to be accomplished by fifty drops or five hundred. We begin with generally two or three drachms spilt on the handkerchief or lint; and we refresh that, or not, from time to time, as circumstances require:" Surgical Experience of Chloroform, Edin., 1848, pp. 16 and 17. The italics are not in the original.
43aCurious arguments are sometimes used in support of the idea of peculiarities and idiosyncrasies. A medical man informed me, one day, that he had seen a patient inhale an ounce of chloroform without any effect. I expressed my opinion that if she had taken the vapour of one drachm into her lungs within four minutes, or the vapour of a little more than half a drachm within two minutes, she would have been insensible; and that the chloroform had mostly evaporated into the room, without entering the patient's lungs. Then, he said, it would have made all of us insensible. Now to charge the air of a moderate sized room of twenty feet square and ten feet high, uniformly with only a grain and a half of chloroform to each hundred cubic inches, so that, if all the crevices were closed, a person inside might, in course of time, absorb about eighteen minims of the medicine, and be rendered insensible, would require nearly fifteen pounds of chloroform.
44The increase of effects of chloroform after the inhalation is discontinued, was pointed out by Prof. Sédillot of Strasbourg and myself almost simultaneously. I explained the circumstance in a paper read to the Westminster Medical Society, on January 8th, 1848, and M. Sédillot announced it to the Academy of Sciences of Paris, on January 10th. My remarks were published in the Medical Gazette of January 14th, and those of M. Sédillot in the Gazette Médicale of January 15th.
45I have reason to conclude that the increased secretion of saliva is caused, not so much by the action of the chloroform on the mucous membrane of the mouth, and the extremities of the gland ducts, as by its action on the capillary circulation of the glands themselves; for on inhaling the vapour carefully by the nostrils, so that none enters the mouth, I still find that there is an increased secretion of saliva.
46London Journal of Medicine, April 1852.
In one of the latest communications of Dr. Marshall Hall to the Lancet, he did me the honour to quote the account of the three following experiments, together with some accompanying remarks from the London Journal of Medicine, and to make the following observation respecting the pages from which he quoted: "I have no hesitation in affirming that the first three pages of this paper are amongst the most able and valuable in physiology, and I beg to be allowed to reproduce them in the pages of the Lancet." (Lancet, April 18th, 1857, p. 397.)
47Edin. Med. and Surg. Journal, vol. lviii.
48Lond. Med. Gaz., vol. xlii, p. 414.
49London Journal of Medicine, April, 1852.
50London Medical Gazette, vol. xlii, 1848, p. 109.
51On the Inhalation of the Vapour of Ether, p. 82.
51aMedical Gazette, vol. xlii, p. 415.
52See l'Union Médicale, 1855, No. 13.
53London Medical Gazette, vol. xli, p. 255.
56London Medical Gazette, vol. xli, p. 75.
56aLondon Medical Gazette, vol. xlii, p. 80, from Western Lancet, and Phil. Med. Exam. April 1848.
58Gazette Médicale, 8 Juillet, 1848; and London Medical Gazette, vol. xlii, p. 211.
59Proceedings of Academy on Feb. 6th, 1849. See London Journal of Med., 1849, p. 307.
60London Journal of Medicine, 1849, p. 324.
61Lond. Med. Gaz., vol. xliii, p. 694.
62London Med. Gaz., vol. xlii, p. 84.
63Bouisson, Traité de la Méthode Anesthésique, p. 398.
64London Med. Gaz., vol. xliii, p. 41.
65Ibid., p. 747, from 1'Union Médicale.
66Lancet, 1840, vol. i, p. 205.
67L'Union Médicale, Sept. 8th, 1849; and Med. Gaz., vol. xliv, p.478.
68Lond. Med. Gaz., vol. xliv, p. 757.
69Journal of Prov. Med. and Surg. Assoc., 1849, p. 698.
70Casper's Wochenschrift, Jan. 12, 1850; and Lond. Med. Gaz., vol. xlv, p. 483.
71Edin. Monthly Journal, April 1850, p. 377.
72Hygiea, October 1850, p. 602.
73Lond. Med. Gaz., vol. xlvi, p. 39.
74Lancet, 1850, vol. ii, p. 21.
75L'Union Médicale, January 29, 1852.
76Medical Times, 1851, vol. ii, p. 98.
77Medical Times, 1851, vol. ii, p. 620.
78Medical Times and Gazette, vol. i, p. 293.
79Medical Times and Gazette, p. 318.
80See a clinical lecture by Mr. Stanley, Med. Times, Nov. 22, 1851.
81Gaz. Médicale, 1852, p. 630, from Medicinisches Correspondenz Blatt.
82Medical Times and Gazette, 1852, vol. ii, p. 531.
83Monthly Journal of Med., vol. xv, 1852, p. 377.
84Lancet, 1853, vol. i, p. 21.
85Lancet, 1853, vol. i, p. 307.
86Med. Times and Gaz., 1853, vol. ii, p. 47.
87Monthly Journal, Nov. 1853 p. 427.
88Since writing the above, I have noted by the watch the time which a surgeon occupied in shaving the perinæum before the operation of lithotomy; it was twelve seconds.
89Medical Times and Gazette, 1853, vol. ii, p. 422.
90Medical Times and Gaz., 1853, vol. ii, p. 449.
92Edin. Monthly Jour., vol. xix, 1854, p. 372.
93Med. Times and Gaz., 1854, vol. i, p. 19, from Med. Zeitung von den Vereine für Heilkunde in Preussen, No. 44, Berlin, Nov. 2, 1853.
94Association Med. Jour., 1854, p. 109.
95L'Union Médicale, 1854, p. 171.
97Association Medical Journal, 1854, p. 315.
98Medical Times, 1854, vol. i, p. 572.
99Medical Times and Gazette, 1854, vol. ii, p. 86.
100Med. Times and Gaz., 1854, vol. ii, p. 390.
102Med. Times and Gaz., 1854, vol. ii, p. 501.
103Medical Times and Gazette, 1855, vol. i, p. 363.
104Edin. Med. Jour., 1855, p. 524.
106Medical Times and Gazette, 1856, vol. ii, p. 442.
107Association Med. Jour., 1856, p. 903.
108Medical Times and Gaz., 1856, vol. i, p. 236.
109Lancet, 1857, vol. i, p. 429.
110Med. Times and Gaz., 1857, vol. ii, p. 171.
111Med. Times and Gaz., 1852, vol. i, p. 627.
112Gaz, Médicale, 1853, p. 304.
113Lancet, 1848, vol. ii, p. 47.
114Bouisson, Méthode Anesthésique, p. 398.
115Casper's Wochenschrift, September 6, 1850; and London Med. Gaz. vol. xlvii, p. 261.
116Medical Times and Gazette, 1854, vol. i, p. 516.
118Chloroform: How shall we ensure Safety in its Administration? Pamphlet. London: 1855.
119See some interesting papers on the value of recumbent position in syncope, by Dr. Richardson, in the Association Medical Journal for 1854. I entirely agree with Dr. Richardson that no kind of syncope commences at the brain, and that, during recovery, the heart always resumes its functions before consciousness is restored. The restoration of the heart's action in ordinary syncope by the re-supply of blood to its cavities, without any alteration in the condition of the brain, was well proved by Dr. Richardson by means of some interesting experiments on animals which I had the opportunity of witnessing.
120Oration before the Hunterian Society. Pamphlet, 1855.
121Hydrochloric acid gas and ammonia are no exceptions to this rule, for they cease to exist as gases so soon as they come in contact with the moist lining membrane of the air passages. Carbonic acid gas will be treated of in another part of this work.
122See Med. Times and Gaz., 1853, vol. ii, p. 562.
124Edin. Monthly Jour., 1853, vol. xvii, p. 220.
125Med. Times and Gaz., 1852, vol. i, p. 627.
126L'Union Médicale, 1850, p. 411.
127Lond. Med. Gaz., vol. xliii, p. 230.
128Medical Times and Gaz., 1856, vol. ii, p. 413.
129Med. Times and Gaz., 1856, vol. ii, p. 478.
129a Ib[id]., 1857, vol. i, p. 559.
131Practical Surgery, 3rd ed., p. 682.
132I never allow of a cork or any such substance being put into a patient's mouth when insensible unless it is well tied to a string, lest it should be swallowed.
133Fourth edit., vol. ii, p. 467.
134It was made by Mr. Matthews, Portugal Street. It was not contrived by me.
135London Journal of Medicine, vol. i, pp. 54, 976.
136See Medical Times and Gaz., 1855, vol. i, p. 361.
137Dr. Watson defends the original name of this complaint, delirium tremens. He says:--"But they who object to delirium tremens appear to see no harm in delirium ferox: whereas it is just as incorrect to say delirium is fierce, as to say that it trembles: it is the patient who is furious, even as it is the patient who trembles." Now, in speaking of a patient, we may speak either of his mind or his body: we may say that a person is learned, or that he is fat. A patient may be fierce on account of the kind of delirium with which his mind is affected, and the term ferox applies both to him and the complaint; but the act of trembling affects only his body.
138Med. Gaz., vol. xli, 1848, p. 102.
139Association Med. Journ., 1853, p. 706.
140See Med. Times and Gaz., 1853, vol. ii, p. 412.
141Med. Times and Gaz., 1857, vol. ii, p. 553, and 600.
142Med. Times and Gaz., 1856, vol. ii, p. 528.
143Brande's Chemistry, 5th ed., p. 1274.
144Lond. Med. Gaz., Feb. 1842.
145On the Inhalation of the Vapour of Ether in Surgical Operations. London, 1847.
146Papers on Narcotism by Inhalation. Lond. Med. Gaz., vol. xli-ii.
149Medical Gazette, vol. xxxix, p. 358.
150Gaz. Médicale, Mars 4, 1848, p. 170.
151Gaz. des Hôpitaux, Juin 18, 1853.
152Medical Gazette, vol. xxxix, p. 414.
154Medical Gazette, vol. xxxix, p. 631.
155Méthode Anesthésique, p. 394.
156American Journal of Med. Science, July 1857, p. 284.
157Annales de Chimie et de Physique, 3ème série, tom. xii, p. 320.
15815, Hanover Street, Hanover Square.
159Bulletin Général de Thérapeutique, t. lii, p. 312.
161Less than an ounce of amylene was poured out, and it was not all used.
162Medical Times and Gazette, 1857, vol. i, p. 84.
163British Medical Journal, March 28th, 1857.
164Bulletin Général de Thérapeutique, t. lii, p. 223.
165Gazette Hebdomadaire, 1857, p. 164.

